


Exercise Might Be a Cancer Drug. Sort Of.

A new study in the New England Journal of Medicine made waves with an almost unbelievable result: a structured exercise program for colon cancer survivors reduced death by 37%:
It’s the sort of shocking top-line result that, if it’s real and replicable, would actually have a massive impact on the way we treat cancer.
The CHALLENGE Trial
The study, called CHALLENGE, enrolled around 900 patients with stage II/III colon cancer who had undergone surgery and completed adjuvant chemotherapy, then randomized them to either a structured exercise program or usual care.
Lots of doctors think that exercise is medicine, so this was a compelling hypothesis to test in a high-risk clinical population.
Even true believers were surprised by the magnitude of the effect: improvement in disease-free survival, fewer new cancers, and lower mortality. Striking.
We need to look at the specifics to understand what it means
You can’t just tell cancer patients to exercise more and expect that’s going to make them live longer.
For a finding like this to be applicable to your own life—or to a patient with cancer—we need to know the specifics:
What type of exercise did they do?
How much did they actually do?
Was the goal total activity or specific functional improvements?
What kind of support did they have?
What was the actual structure?
In my post on advice to young doctors, I wrote about one of the most important things I’ve learned in medicine: amateurs talk strategy; professionals talk logistics.
If you don’t understand the specifics, your advice will be unhelpful and your program, for yourself or your patients, is likely to fail.
The Top Line Result Looks Almost Too Good
On the surface, this study doesn’t pass the smell test. The results seem too good to be true.
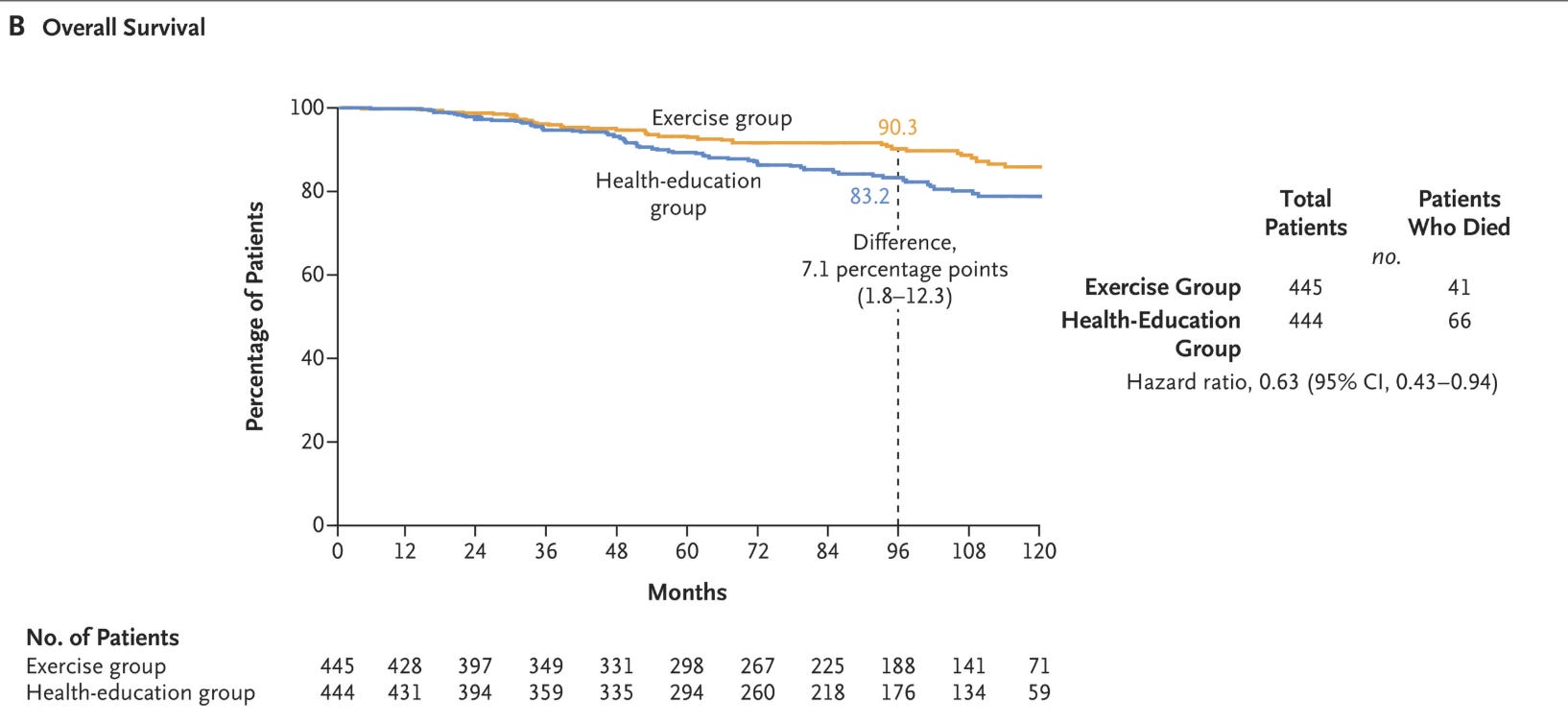
Compared to usual care, the intervention group had a 37% reduction in all-cause mortality.
Put another way: if you put 14 cancer patients on this exercise program, you prevent one death.
The relative risk reduction for overall death (HR 0.63; 95% CI, 0.43 to 0.94) was even greater than the reduction in the composite endpoint.
Exercise also seemed to reduce recurrent colon cancer (65 vs. 81 patients) and new primary cancers (23 vs. 42 patients).
The authors concluded that the 3-year program “resulted in significantly longer disease-free survival” and had “findings consistent with longer overall survival.”
As John Mandrola put it in his excellent Sensible Medicine editorial: this type of benefit rivals the mortality reduction we see with Herceptin in HER2+ breast cancer.
The Exercise Intervention… Wasn’t That Intense
If you read the supplementary appendix (and you should), you’ll find this wasn’t a program of CrossFit, marathon training, or HIIT.
The “exercise” was largely brisk walking: a target of 150 minutes per week of moderate-intensity aerobic activity, with personalized coaching sessions and regular phone calls.
Many participants never completed follow-up treadmill or 6-minute walk tests. Adherence was suboptimal. And because the analysis was intention-to-treat, even people assigned to exercise who didn’t follow through were still counted in the exercise group.
But this is actually one of the most compelling parts: the type of exercise people did makes this study more applicable to real life. It’s doable.
Most people don’t like intense exercise. If the bar were too high, this trial wouldn’t apply to a general population.
Instead, the intervention was realistic. This increase in physical activity was the equivalent of:
45 to 60 minutes of brisk walking, 3–4 times per week, or
25 to 30 minutes of jogging, 3–4 times per week
The difference in moderate-to-vigorous physical activity over 3 years was about 5.2 to 7.4 MET-hours per week - roughly 1.5 to 2.25 hours of walking at 3 mph.
It’s a very doable bar.
A Question of Biological Plausibility
So is this biologically plausible?
That depends on what you believe exercise actually does.
If your model is that exercise improves cardiorespiratory fitness, the results are harder to interpret. You’d expect a clearer impact on VO₂ max or other functional markers if fitness were driving survival.
But the fitness improvements were tiny:
VO₂ max improved by just 0.6 mL/kg/min - a modest change with unclear clinical significance
6-minute walk distance increased by 30 meters
No change in weight or waist circumference
These are not the kinds of changes that typically reduce mortality by a third.
This is the longevity guru model: you train to increase VO₂ max because it correlates with mortality in population studies. From that lens, low-intensity exercise that doesn’t raise VO₂ max barely counts.
(Zone 2 purists would argue 150 minutes a week barely hits the minimum dose for mitochondrial adaptations.)
But What If the Benefit Comes From Somewhere Else?
If your model is that even low-level physical activity improves insulin sensitivity, metabolic health, and inflammation, the story changes.
You don’t need intense training to:
Reduce blood glucose
Increase GLUT4 expression in skeletal muscle
Improve insulin regulation
The authors suggest several possible mechanisms by which exercise may benefit cancer outcomes:
Increased fluid shear stress
Improved immune surveillance
Altered metastatic microenvironments
In other words: walking might not raise your VO₂ max, but it could still shift your metabolic milieu.
There’s something to this - the exercise group also had major improvements in quality-of-life scores.
So maybe the benefit is physiologic, even if it doesn’t show up in traditional metrics.
Think back to the London transport workers study. This classic observational study found that bus conductors (on their feet all day) had far lower heart disease rates than drivers (who sat all day), despite similar diets and backgrounds.
Maybe movement matters in ways we’re not great at measuring.
Or Maybe It Wasn’t the Exercise at All
Let’s be honest: this wasn’t just a movement intervention.
It was a human connection intervention.
Regular contact with trainers
Frequent phone calls
Accountability
Encouragement
Support
We’ve seen this before. STRONG-HF showed improved heart failure outcomes not through a new drug, but by simply seeing patients more often and titrating meds.
Maybe the secret sauce in CHALLENGE isn’t walking - it’s being supported.
People do better with connection.
Now, to be fair, the authors note that other oncology trials with frequent psychosocial contacts didn’t show survival benefits. So maybe it’s not just the attention.
But it’s hard to separate the two.
The Trial Design Leaves Questions
There are good reasons to be skeptical:
The trial took 15 years to complete, introducing major heterogeneity.
Activity levels were self-reported, which is a notoriously unreliable method.
The population was healthier and higher-functioning than most post-chemo colon cancer patients.
Event rates were lower than expected. The study was underpowered at 3 years.
Adherence was low.
The intervention group received significantly more attention, introducing potential performance bias.
One critique I’ve heard that I don’t buy: recurrence curves diverged early, but mortality curves didn’t until 4 years in. But that actually makes sense. Fewer recurrences would appear early. Death takes longer.
What Should We Make of All This?
I think two things are true:
Exercise is good.
It improves metabolic health, prevents chronic disease, and might reduce cancer recurrence.
This trial almost certainly overstates its effect.
Not because it’s wrong, but because it wasn’t just exercise and the effect size is suspiciously large.
That said, I’ve changed how I talk about walking with patients from this.
My Mental Model of Physical Activity
I think of movement in four pillars:
Not being sedentary (e.g., 10,000 steps/day)
Low-level aerobic (e.g., Zone 2)
High-intensity cardio (e.g. sprints)
Resistance training to build muscle and strength
I encourage people to touch each of those pillars, but I emphasize:
Consistency over optimization.
If you hate cardio but love lifting, I’d rather you lift three times a week than skip sessions trying to force a perfect mix.
Final Thought
We often try to separate the biological from the behavioral. The physiological from the psychosocial. But that’s not how humans work.
If we tell patients that walking daily cuts cancer death by 30%... it’s probably an oversell.
But if we tell them that moving your body, staying connected, and being cared for can change your life?
That might actually move the needle.
Oh, and the best exercise program to prevent cancer?
It’s the one you’ll actually do.