

Getting ready for the next pandemic

You’re probably reading that title and wondering why I’m getting so far out ahead of myself. After all, we haven’t finished this pandemic yet.
While we’ve learned a great deal about the various aspects of COVID-19 and the SARS-CoV-2 virus - testing, treatments, vaccines, non-pharmacologic interventions - there are a lot of lessons that aren’t necessarily virus-specific that might make us better prepared for the next pandemic.
And make no mistake - the next pandemic will come.
It’s only a matter of time.
Pandemics are not new
Pandemics may feel like they’re new, but that’s only because we used to call them by a different name: plague.
Plagues have been a part of the human experience since the dawn of civilization, more than 12,000 years ago. After agriculture and animal domestication enabled larger, denser, and more permanent human settlements, we’ve been dealing with plagues.
Close contact with animals led to the emergence of zoonotic diseases - human infections caused by a pathogen that lives in animals. Denser settlements enabled rapid and widespread infection. You’re probably familiar with a lot of this history.
The Justinian Plague in the 500s AD and the Black Death in the Middle Ages were caused by a bacteria called Yersinia pestis.
Smallpox devastated North American indigenous people.
The 1918 flu pandemic killed over 50 million people.
HIV is considered by some to be a pandemic that has killed more than 37 million people.
And that’s only a small sample of pandemics past. Unfortunately, things are accelerating.
The past 20 years have been an unprecedented pandemic explosion
Think about some of what we’ve seen since the dawn of the 21st Century.
SARS in 2002 - emerging from a civet to cause a near pandemic that was only stopped with draconian public health measures.
The “swine” flu H1N1 in 2009 killed 284,000 people globally.
Mosquito borne diseases like Chikungunya and Zika emerged in 2014 and 2015 and both reached pandemic status.
And that doesn’t include the pandemic-like emergencies of the past few years. I’m thinking of Ebola, a hemorrhagic fever likely transmitted by bats, which caused a huge outbreak in Sierra Leone, Liberia, and Guinea just a couple of years ago. And then there is MERS, a coronavirus like SARS and SARS-CoV-2 which came from camels. MERS didn’t quite reach pandemic status since it doesn’t seem to be all that as contagious, but it’s something to be worried about because it’s quite deadly.
So it means that the end of the COVID-19 pandemic - which is currently in the midst of its 4th surge, in case you haven’t seen the unfortunate new spike in case numbers - doesn’t lead to a world where we will never think about wearing masks or freaking out about superspreader events.
Improving vaccine infrastructure is how we will be better prepared next time
If nothing else, the experience with COVID-19 has taught me that stopping a pandemic is really hard!
Wearing masks, social distancing, restrictions on gatherings and travel aren’t perfect means of preventing viral spread. And they also don’t come without unintended consequences. In exchange for reducing viral spread, we screw up our kids lives, gain weight, and feel lonelier.
The only thing that’s brought a possibility of light at the end of the tunnel is the miraculous development of incredibly effective and safe vaccines.
So when we think about our preparedness, the smart thing to do is to invest in an infrastructure that allows for the speedier development, testing, and manufacturing of vaccines when the next pandemic inevitably hits.
There’s a super interesting paper that I just came across by Florian Krammer, a virologist at Mount Sinai, about how we can start getting ready for the next pandemic now by improving our vaccination infrastructure.
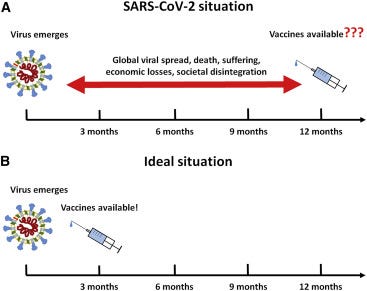
Just imagine all the suffering, death, and devastation we might have been able to prevent if we had a safe and effective vaccine available in March of 2020:
Part 1: start with the respiratory viruses
While we don’t know exactly what type of pathogen is going to start the next pandemic, we’ve learned that we need to be most worried about respiratory pathogens that spread quickly - part of the reason COVID has been so devastating is how easily it spreads.
We can identify families of viruses with the highest pandemic potential and select 50-100 different viruses to build vaccines against.
“The idea is that once viruses are selected, vaccines can be produced in different platforms and tested in phase 1 and phase 2 trials with some of the produced vaccine being stockpiled. This would likely cost 20–30 million US dollars per vaccine candidate resulting in a cost of 1–3 billion US dollars. If a new virus hits, the vaccine closest to the new strain is selected, a strain change is performed, vaccine production starts immediately, and phase 3 trials are initiated within a month.”
Part 2: understand surrogate markers for immunity
There’s been a lot of news about neutralizing antibody titers in response to different viral strains or how T cell activation may be the vital part of establishing lasting immunity.
But unfortunately, when it comes to SARS-CoV-2 and other coronaviruses, we don’t have a solid understanding of which surrogate markers truly predict immunity. As I think I’ve said before - who cares what your antibody titers are if you die of COVID? And who cares if you have no antibodies if you have viral immunity?
Studying this in detail so that we understand it could speed up vaccination trials even further:
“It is likely that neutralizing antibodies against coronaviruses do in fact correlate with protection in humans, but since this has not been shown in adequately sized and diverse populations, we cannot base vaccine licensure on a correlate and must perform much larger, more labor-intensive, and longer field efficacy studies. However, having a correlate of protection for a closely related virus and animal data suggesting protection based on that correlate as well would allow us to base short and much smaller phase 3 trials on immunogenicity readouts alone.”
Part 3: boost vaccine production capacity ahead of time
It’s a real challenge to go from producing zero of something to producing billions of something very quickly if you don’t have the factories ready to go.
This will require up front investment in new factories that will likely remain dormant most of the time but need to be maintained to start production quickly in the event of a new pandemic.
This expensive process - which needs to be supplemented with secure production facilities and supply chains for syringes, vials, and storage containers - is the only way to ensure that our production capacity is ready when necessary, and that we minimize the chance of some of the COVID vaccine production issues that we’ve seen.
We need take action in productive ways to truly learn from this pandemic
Improving vaccination infrastructure is clearly only part of adequately preparing for the next time:
“Many measures need to be taken to mitigate or even prevent the next pandemic. These include better surveillance systems, global pandemic response plans that are executed, development of broadly acting antivirals, and further development of diagnostics and non-pharmaceutical interventions.”
But given our experience with COVID, I think that improving vaccine readiness may be the most important thing that we can do moving forward.
We’ve seen unprecedented societal disruption across disciplines from this pandemic. And the damage isn’t over yet.
Because of how poorly we’ve done with the draconian measures required to truly stop the spread of a contagious and deadly respiratory virus, developing the best vaccination plan we can really does seem to be the only way out when this happens again.
Thank you for reading! If you’re enjoying my newsletter, please consider sharing with your friends and family and encouraging them to subscribe!
I always appreciate any feedback or thoughts you might have. You can reply directly to this email to reach me directly.