




The link between inflammation and heart disease is quite well established.
We know this for a few reasons:
Looking at arteries of people with heart disease shows inflammatory cells are present in vascular plaque
People who have diseases that lead to chronic inflammation (like lupus or HIV) have accelerated heart disease
Some medications that lower inflammation have a beneficial impact on heart disease risk
And so the recent news that an old anti-inflammatory medicine called colchicine was just approved to reduce heart attacks does not come as a surprise to me.
Colchicine is an old medication with a long track record
Colchicine has been around forever.

It’s probably best known as a treatment for gout, but it’s also used in other diseases like pericarditis and Familial Mediterranean Fever.
Colchicine has a long track record of safety, but there are a couple of risks associated with it.
Colchicine causes diarrhea in a fair number of people who take the medication.
This isn’t a side effect of the medicine as much as it is a direct effect of the way that it works. [For those interested, colchicine inhibits cell division because it impairs microtubule formation - the fastest growing cells in the body are the brush border cells of the intestine, and so if they can’t grow as quickly, you’ll have intestinal malabsorption, which leads to diarrhea.]
If someone starts colchicine on you, they should give a heads up, because the diarrhea can be pretty alarming and cause people to stop the medication.
But that only happens a small amount of the time. Otherwise, for people who don’t have significant kidney disease, colchicine tends to be safe and well tolerated, with very low risk of serious side effects (like low white blood cell counts or muscle aches).
The impetus to approve colchicine for heart disease comes from the LoDoCo2 trial
LoDoCo2 is a trial looking at the impact of low dose colchicine on the risk of heart attack, stroke, death, and need for a stent.
LoDoCo2 comes as a follow up to LoDoCo and COLCOT, both of which had similar results.
LoDoCo was too small to draw conclusions from, and COLCOT looked mostly at patients right after a heart attack, who tend to be more actively inflamed than patients with stable heart disease.
LoDoCo2 studied patients with known heart disease who had been stable for about 6 months and compared the impact of colchicine to placebo.
The results were quite impressive:

The curves diverge quickly and they keep diverging over 5 years.
This suggests an additive benefit to long term colchicine treatment in reducing heart disease risk.
And so while the results here are pretty cool - a drug that has a long track record of safety and effective use lowers the risk of heart disease, I struggle with the use case.
Exactly who is this medicine for? Should we treat every single person with heart disease with low dose colchicine?
I have a hard time knowing what to do with colchicine for heart disease, even after LoDoCo2 and COLCOT
Most heart disease is driven by blood pressure and lipids.
And while we can just throw colchicine onto a med list for every heart disease patient, it would reduce polypharmacy quite a bit to have a better sense of who is most likely to benefit.
The limit for many patients in getting optimal treatment is that they are on a lot of pills. At a certain point, just adding more medications creates additional problems.
While it’s great to have more tools in our toolbox, it would be even better if we have a sense of how to selectively use these tools.
Plus, we don’t know if colchicine adds much on top of optimal blood pressure and lipid management - if the LDL is 40 (or the apolipoprotein B is 35) and the blood pressure is 115/75,
After all, these trials didn’t tell us very much about how well the classic risk factors were controlled in the patients studied.
We don’t have information about blood pressure, LDL, or glucose control, so I don’t know how colchicine is compared to optimal treatment of these other risk factors.
We also don’t have a colchicine biomarker to gauge effectiveness
When you treat lipids, you aim for an LDL or apoB goal.
When you treat blood pressure, you have very clear aims.
But I don’t know how to measure the effect colchicine therapy, or even guide who is most likely to benefit.
We have very limited information about their level of inflammation. LoDoCo2 doesn’t give us any information on their C-reactive protein (a marker of inflammation often used in assessment of heart disease risk).
COLCOT shows us that CRP levels got better both in the group treated with colchine as well as the group treated with placebo, making it hard to develop a biomarker to guide treatment success:

The other caveat here - why doesn’t colchicine save lives even if it prevents heart attacks and strokes?
When you look at the adverse events in LoDoCo2, you see something curious. More people died of noncardiovascular death in the colchicine group than in the placebo group:
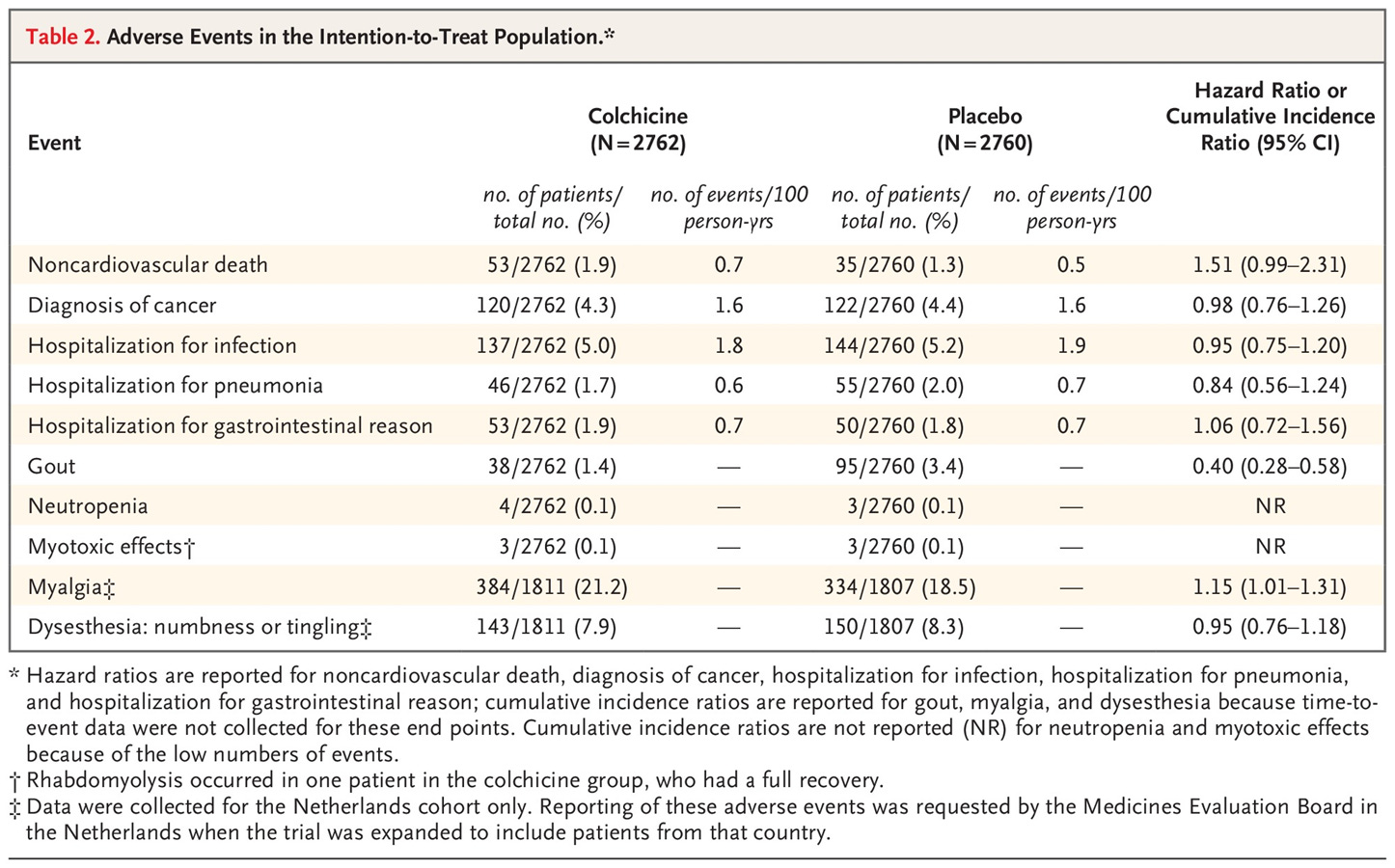
You can certainly look at the overall numbers and say that statistical significance was not met, therefore it’s not a problem, but that confidence interval barely crosses one, and so I’m inclined to worry about the risk here.
I’m not suggesting that colchicine kills you, but I am a bit surprised to see this.
Longer term follow up may prove that this is just an anomaly driven by chance. But it’s certainly not something I would ignore. Death is kind of an important outcome to study.
At the end of the day, I think colchicine is a nice option to have in our toolbelt to prevent heart disease
I will continue to focus my cardiovascular prevention on the classic stuff - blood pressure, lipids, blood sugar/diabetes/metabolic syndrome - but I will keep colchicine in mind for select patients.
My ideal use case is a patient who is optimally treated for the classic stuff and still has residual inflammatory risk.
I use a high sensitivity CRP to suggest elevated inflammatory risk - optimal is under 1.
If a patient has a CRP over 1 and is otherwise well treated, that’s where colchicine may have a role.
It’s important to keep in mind, however, the CRP is driven in part by insulin resistance and metabolic syndrome, so this often comes down with lifestyle changes (more exercise, less junk food, and weight loss).
I think of colchicine as a complement to rather than a replacement for our standard heart disease treatments.
It’s not for everyone, but it also has a role in the carefully selected patient.