
Making stress tests obsolete

We perform 8 million stress tests a year in America.
I would wager that a large portion of the people reading this newsletter have either had a stress test themselves or know someone who’s had a stress test - it’s one of the bread and butter tests in cardiology.
But there’s an emerging new technology that has the promise (to investors at least) that it’s going to render stress tests obsolete.
That technology is called CT-FFR, and a company called HeartFlow just raised over $200 million as they scale up their implementation of this technology.

This is a big deal because of how it may impact the noninvasive cardiac testing that we do; because heart disease is so common, this is going to impact a lot of patients.
What’s the point of a stress test?
The purpose of a stress test is to help figure out if you have a severe blockage in one of the arteries of your heart.
A stress test assesses the plumbing of the heart, it doesn’t tell you that much about structure, function, valve problems, or electrical issues.
The name stress test comes from the fact that these tests put additional demand on the heart, either through the form of increased bloodflow or increased workload, with the goal of figuring out if there’s a severe blockage in one of the arteries.
But the images in a stress test (whether it’s an EKG, nuclear tracer, or echocardiogram) aren’t actually looking at the blood vessels themselves, they’re using surrogate markers to infer information about blood flow.
There are two major issues with stress testing.
When you use a surrogate measure of blood flow, you don’t actually know for certain whether a blood vessel is clogged. With an abnormal test, you often need to obtain some type of anatomical imaging to fully confirm it.
A stress test is incapable of picking up a blockage that’s mild or moderate in severity. The stress test is only capable of picking up a severe blockage. If a blockage is there but it’s not severe, the stress test can’t tell.
The reason it’s not a catastrophic flaw that stress tests only find severe blockages is that blockages only cause symptoms when they are severe.
And so if you’re using a stress test as a diagnostic tool for symptoms, you could make the argument that you only need to know whether there’s a severe blockage causing symptoms (I wouldn’t make that argument, I’m just saying that you could make it).
Stress tests aren’t great - there are a lot of false positive and false negatives, and that leads to downstream consequences
It’s obvious what happens if a stress test doesn’t pick up a blockage because it wasn’t severe enough to compromise blood flow - you don’t know about it, can’t treat it, and may give false reassurance to someone who should be medically treated for heart disease.
But very often an abnormal stress test leads to an invasive procedure called a cardiac catheterization (you may have heard it called an angiogram, which just means a picture of blood vessels).
This is where an interventional cardiologist places a catheter into a blood vessel in either your wrist or your groin, moves it up to the heart, injects dye into the blood vessels around the heart, and takes x-ray pictures.
These pictures let us directly visualize the blood vessels, so you can see any degree of blockage and even put a stent in to fix a severe one (the decision about whether to put in a stent can be complicated and is a subject for a different newsletter).
But a problem with the catheterization is that it’s invasive (which carries risk of causing a heart attack or a stroke), requires anesthesia, is expensive, and sometimes unnecessary.
So anything that improves the diagnostic accuracy of a noninvasive test may mean that we do fewer unnecessary invasive procedures
Enter the coronary CTA - a noninvasive angiogram that lets us directly look at the blood vessels around the heart
One of the most exciting technological advances in cardiology over the last decade or so is a test called a coronary CTA, a test that uses CT scan technology to image the blood vessels around the heart.
The advantage of a CTA over a stress test is that the CTA can let you see if there are any blockages or calcium buildup in the arteries around the heart, not just severe ones.
And if there are any blockages, the CTA can also tell you how severe they are, with a margin of error.
This is a game changer because we can directly look at someone’s anatomy to diagnose and quantify the presence and degree of heart disease present.
CTAs also help us more carefully select which patients have severe blockages and might benefit from an invasive procedure.
The major problem with the CTA is that there are some blockages that are indeterminate in nature, i.e. they are somewhere between moderate and severe, but the scan does not have the resolution to decipher between the two.
That makes it hard to sort out whether a patient’s symptoms are due to a blockage in the arteries or due to something else.
CT-FFR technology promises to eliminate the ambiguity of how severe a blockage is
This is where the HeartFlow technology comes in.
They use fluid dynamics and complicated mathematical modeling to figure out more precisely whether a blockage is actually moderate (in which case symptoms are unlikely to be related to a blockage and a stent plays no role), or actually severe (in which case the symptoms are likely a result of a blockage and a stent may be helpful).
This technology is modeled on a tool that interventional cardiologists use during catheterization, called FFR, or fractional flow reserve.
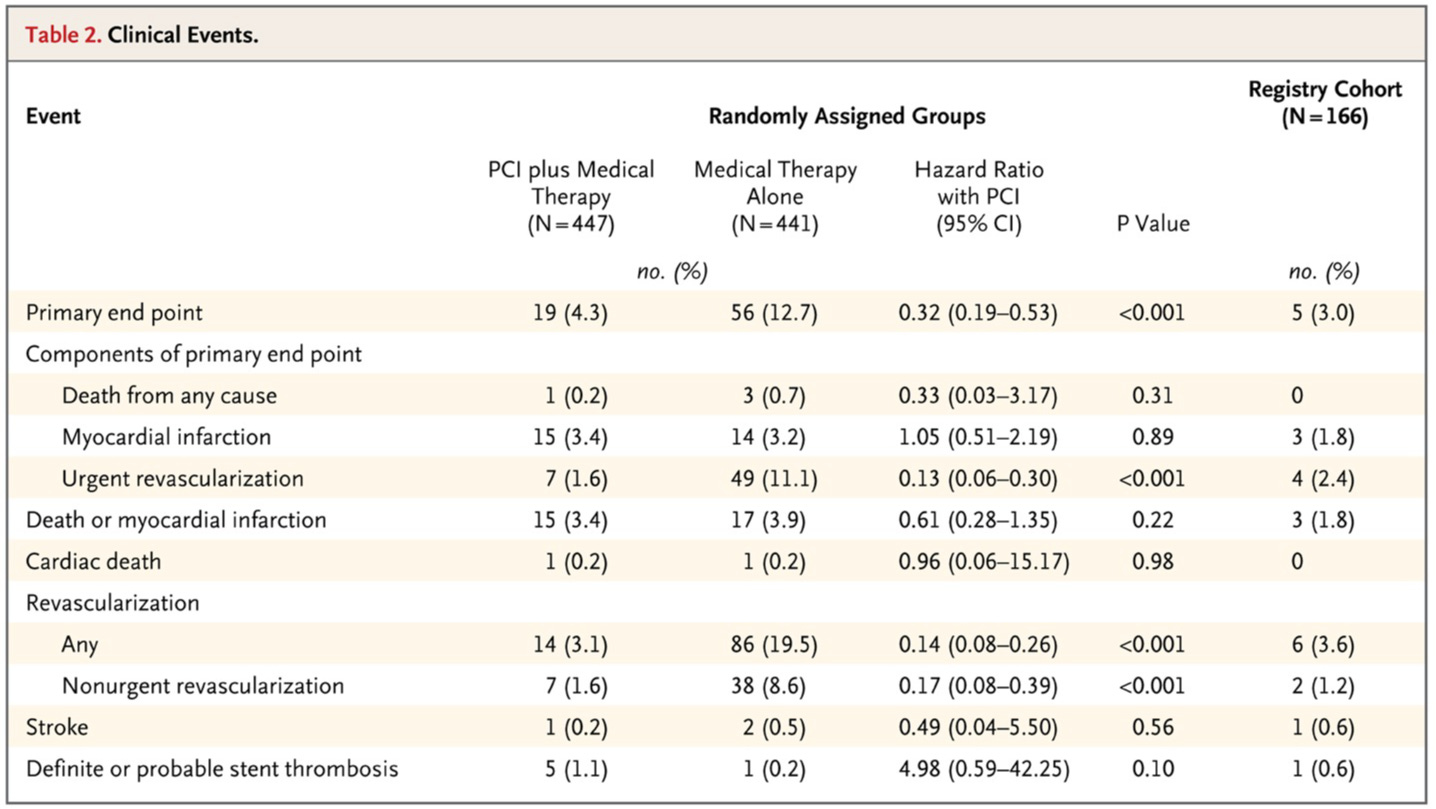
FFR was made famous in the world of cardiology after the FAME-2 trial, which showed a reduction in major adverse cardiovascular events by using FFR technology to make decisions about whether to put in stents for blockages that looked intermediate (between moderate and severe) on visual inspection:

Being able to use FRR noninvasively holds tremendous potential for diagnostic accuracy and reducing unnecessary procedures.
And you add that layer on top of the CTA technology, which lets you visualize the presence of any heart disease, not just heart disease severe enough to cause symptoms, and you can get the best of both words - early detection and more precise diagnostic discrimination.
In theory, CT-FFR is a fantastic test. If you believe the full narrative of what this company is selling, they may eventually make nuclear stress tests obsolete
This technology is pretty amazing.
HeartFlow published some preliminary data from a study called PRECISE, where they looked at use of CT-FFR compared to traditional testing and found a big reduction in pointless invasive testing, which is the intuitive result that you’d expect from this type of test that directly looks at the anatomy.
But that’s a small study that didn’t show any impact on the things that we care about most: death, heart attacks, or death from cardiovascular causes:

I’m pretty uncertain how much impact this technology is going to make, for a handful of reasons
I don’t really know where this is going to end up, and whether CT-FFR is going to make stress testing a thing of the past, for a few reasons:
Doctors are prolific rent-seekers, and stress testing is pretty lucrative
You get way more information from a stress test than just whether it’s positive or negative - you can see exercise capacity, heart rate response, blood pressure impact
A stress test lets you see if stress on the heart replicates symptoms that a patient is feeling
CTAs are of limited use in patients with kidney problems, because of the risk from contrast during the scan, and patients with kidney problems are an increasingly important group to assess for cardiovascular risk
FFR technology isn’t actually that big a deal. The only benefit in the FAME-2 trial was fewer people going for stents. There was no impact on death or heart attack prevention:
The counterargument to that doubt is pretty simple:
There’s already some data to suggest the CTAs improve patient outcomes. Adding FFR technology to an already useful test promises even more utility
There’s a lot on the line with how this plays out.
We’re talking about a lot of tests for a lot of people. That means a lot of people will have their treatment adjusted based on how these tools end up being used.
And you can’t forget that there’s big money to be made with all this testing because heart disease is so common and so serious.
Understanding what these tests are and, perhaps more importantly, what they are not is ultimately vital to empower you about what tests your doctor is sending you for.