




The question “what is long Covid?” should be easy to answer.
After all, we’ve had hundreds of millions of infections worldwide and by some estimates, about 65 million long Covid cases.
Unfortunately, I don’t think that we know very much about it. I’m afraid that long Covid has been poorly studied, with a lot of low quality research flooding the zone with nonsense.
And so, at least right now, long Covid is poorly understood.
But that hasn’t stopped a lot of people from having strong opinions about it.
On one hand, you have the fear mongers who talk about long Covid as an unstoppable societal plague affecting millions, a ticking time bomb about to cripple the healthcare system at any moment.
On the other hand, you have a group of people who think that everyone with “long Covid” is either insane or full of crap, displaying an impressive amount of condescending dismissiveness towards a group of people who are truly suffering.
If you aren’t dealing with it personally and you don’t know people who are dealing with it, it’s tempting to become persuaded by the loudest voices in the room and either think long Covid is nonsense or spend your life afraid of getting Covid because of the risk of becoming a long hauler.
I don’t really believe either of those ends of the spectrum are right based on my own day to day experience.
Actually taking care of long Covid patients changes your perspective on what this disease really is
I have a few patients who are suffering from terrible symptoms after dealing with Covid infection.
I think it’s pretty difficult to be a doctor in clinical practice and still get sucked into any of the political nonsense that follows this group of people around.
Here’s what I mean by that:
Almost everyone who get Covid today has no long term (or even medium term) impact. They have mild symptoms, don’t require medication, and recover fully. When they’re done being sick, they go back to their regular life.
The people who are screaming that long Covid means the sky is falling are wrong. Most people don’t need to be worried, and the absolute risk of getting any long term sequelae is astoundingly low.
But then there’s the incredibly small minority of people who have a very different experience. Some of these folks are really suffering, and we haven’t figured out what’s going on or what we can do to help them.
And this group doesn’t have the medical comorbidities and Axis II psychiatric disorders that long Covid minimalists suggest - many of the long Covid patients I’ve seen are normal human beings who weren’t chronically ill before this happened.
Long Covid patients have a lot of frustrating interactions with the medical system
I think the reaction that a lot of doctors have when they see “long Covid” on a chart is similar to the way they react to “chronic fatigue syndrome” or “fibromyalgia” or “chronic Lyme disease.”
There’s the sense that you don’t have much to offer, and that it’s going to be a frustrating visit for both patient and provider.
But this phenomenon - a person who is suffering greatly in a medical system ill equipped to help them - isn’t new to long Covid.
If you aren’t familiar with this side of medicine, it’s worth reading Ross Douthat on his experience with a mysterious chronic illness, which he’s chronicled in a series of columns in the New York Times:
By reading Douthat, you can see the way that chronic illness that doesn’t fit into a neat diagnostic box can cause a lot of suffering and a lot of frustration.
There’s a lot that we don’t know in medicine, and it’s easy as a physician to be arrogant or dismissive about the things that are beyond our understanding.
And long Covid, whatever it is, is definitely beyond our current understanding.
Long Covid comes in 2 different flavors in my experience
When you read review articles on long Covid (sometimes called Post Acute Sequalae of Covid-19, or PACS), you’ll be struck by how many potential different things have been reported to be wrong in these patients.
It almost seems as though every single organ system can be compromised, which causes confusion about how to make a diagnosis:

My experience is that there are two predominant clinical subgroups:
A group that reports their predominant symptoms are brain fog, fatigue, and cognitive dysfunction. They report extreme exhaustion and are sometimes unable to complete their own activities of daily living
A group that reports symptoms of lightheadedness, palpitations, dizziness, and fast heart rate. This group tends to be extremely sensitive to positional changes like going from lying down to sitting or from sitting to standing up.
Patients across both groups tend to report shortness of breath with exertion and sometimes chest discomfort (which is often why they end up in my office).
And it’s not like the groups are completely mutually exclusive, but my clinical experience is that most people fall into predominantly one of these groups. Even when other symptoms exist, they seem to occur in concert with one of the two major themes.
I haven’t seen anyone who I suspect to have long Covid without symptoms from either bucket.
Despite symptoms that are well characterized, nobody really understands the physiology
There are a few major theories about what’s going on in long Covid according to the review papers:
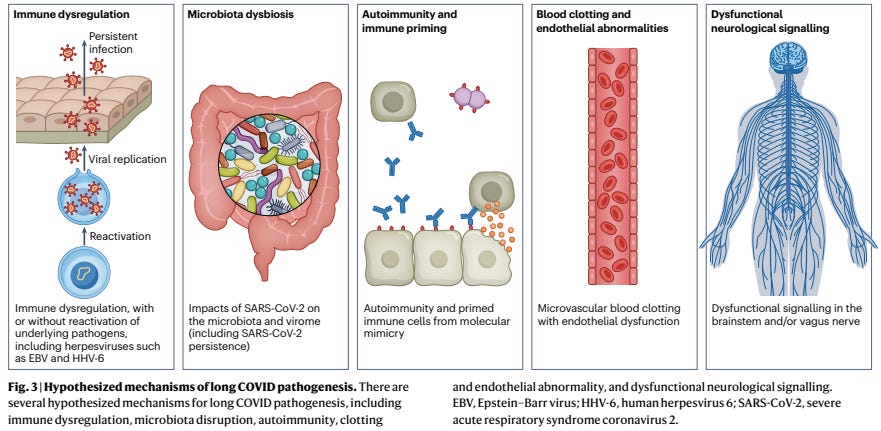
But some other disorders may hold clues to understanding long Covid and considering practical steps to treat it.
Chronic Fatigue Syndrome
You may be familiar with chronic fatigue syndrome (now called myalgic encephalomyelitis/chronic fatigue syndrome, or ME/CFS), which is thought to be due to reactivation of viruses such as EBV or HHV-6, and seems to have a lot in common with the subgroup of long Covid patients dealing with brain fog and extreme fatigue.
These reactivated viruses occur as a consequence of immune dysregulation and may lead to dysfunction of our mitochrondria, which impair energy production.
If energy production in our cells is impaired, you can imagine how fatigue and cognitive dysfunction might result.
Since ME/CFS is both so debilitating and also so devoid of treatments, it’s easy to feel helpless here.
We do have some ideas about what may help to treat dysfunctional mitochrondria, however - low level exercise, which is exactly what I recommend to my patients as their therapy, with varying degrees of success.
But while the ME/CFS-like clinical syndrome explains the brain fog and fatigue group, it doesn’t really explain the lightheadedness/palpitations group, whose symptoms really seem to be more in line with a medical problem called POTS, or postural orthostatic tachycardia syndrome.
Postural Orthostatic Tachycardia Syndrome (POTS)
POTS is the single most common long Covid manifestation that I see, and it’s not even close.
POTS is most simply understood as a problem that humans experience as a consequence of walking upright.
Gravity causes blood to pool in our legs, which reduces the return of blood back to the heart when we are upright.
That causes a drop in blood pressure, which leads to a reflexive increase in heart rate.
With POTS, these normal responses are exaggerated and lead to severe lightheadedness, palpitations, and sometimes even passing out.
The treatments here start in a non-pharmacologic way - sodium supplementation, increased hydration, and compression stockings.
If that fails, the next line of therapy depends whether the predominant symptom is palpitations (in which case you treat with medicines that slow down the heart) or lightheadedness (in which case you treat with medicines that raise blood pressure).
And there’s also an overlap between POTS and an entity called mast cell activation syndrome (or MCAS), which is a disorder of the cells that release histamine that causes symptoms mimicking an allergic reaction.
MCAS is often treated with medications like Pepcid.
Luckily, POTS usually responds to fairly straightforward therapy, as detailed above.
We need to briefly talk about the microclots hypothesis
There’s a hypothesis that some of the multi-system involvement here is caused by tiny blood clots caused by damage to the cells that line our blood vessels (called endothelial cells).
This is a challenging hypothesis to test because there aren’t great diagnostic tools for microclots. Adding to the challenge is the risky nature of empiric treatments for this.
While the other interventions I mentioned above are fairly benign (salt supplements, compressions stockings, beta blockers), the treatment for blood clots is blood thinners.
These medications carry risks of bleeding that aren’t trivial.
I struggle with the idea of “just try something” in this case. The decision to put people on blood thinners without any proof of clotting, method of measuring the effectiveness of your treatment, or anticipated end date makes me concerned.
Long Covid is a hard topic to study and that’s why there’s some much confusion
Long Covid is hard to study because so many people have had Covid (many people more than once) and the symptoms are nonspecific and don’t clearly have a temporal relationship to a viral infection.
It’s going to be a long time before we understand this well, if we ever do.
The approach of treating symptoms (“just try something”) makes sense to me when the treatments are low risk.
And while you’ll read some reports about vaccination or antiviral therapy as a treatment, the studies on this are too low quality and too confounded to draw any conclusions, so these treatments are not in my therapeutic arsenal.
I’ll leave you with this - I believe long Covid is real and can be quite debilitating. But most people don’t get long Covid, and many of those who do get better.
In this case, however, when my patients get better, I’m not totally sure whether it’s because of medicine or in spite of medicine.