


Why was I wrong about blood transfusions?
A look at the MINT trial

Arguably the most challenging part of medicine is distinguishing between correlation and causation.
A lot of research is done observing that there’s a relationship between thing 1 and thing 2. But it’s really hard to untangle whether thing 1 causes thing 2, or whether it’s just a marker for something that causes both of them.
The only way to sort that out is with a randomized controlled trial, which is why I spend so much time on this newsletter writing about this topic.
At the same time, we all have our own preconceived notions about what we expect trials asking causation questions to show when they’re done.
These expectations come partly from the studies that have already been done and partly based on our understanding of disease.
Trial results often deviate from our expectations, and when they do so, it’s worth asking the question, “why did I get it wrong?”
Today, I’m going to talk about the MINT trial, the latest personal example I can share about a time when I thought a clinical trial would show one thing, and I was wildly off base.
The MINT trial looked at the topic of blood transfusions, which has a long, consistent track record in the medical literature
The history of randomized trials on blood transfusions is pretty boring - less has always been shown to be the same as more.
This has been consistent across populations - during surgery, when having GI bleeding, ICU patients - doing more transfusions rather than fewer transfusions is clearly not better and may even be worse.
This was even true in heart attack patients, at least in a pretty small trial.
When the data on something is this consistent across populations and clinical scenarios, it’s quite a powerful argument for a strategy or treatment.
It’s really interesting that blood transfusions don’t look better as a treatment.
After all, anemia is consistently linked to bad outcomes regardless of what disease you’re looking at - the lower your blood counts, the worse you do.
Transfusions correct anemia efficiently and effectively.
But more transfusions to reach closer-to-normal levels of hemoglobin doesn’t make people feel better or live longer (and if we’re being honest, seems like it probably harms most patients).
This has to do with the fact that transfusions aren’t just replacing red blood cell carrying capacity. They come with risks like infection, fever, and heart failure - there just isn’t a free lunch here.
So the mental model that I’ve been practicing with is that most patients with anemia do worse because they’re more chronically ill, not specifically because they’re anemic.
And so when I heard about the MINT trial, I assumed it was going to be more of the same - another data point that more transfusions aren’t better and might be worse.
MINT tested transfusion strategies in heart attack patients - and no, this wasn’t a dumb idea
It’s pretty easy to read that last section and think that there was no point in running a trial like MINT - the evidence has been clear, and we’ve already looked at this specific group of patients with unimpressive results.
But the people who designed this trial aren’t idiots.
They’re smart doctors who are convinced that there remains a legitimate clinical question about whether patients having heart attacks have high red blood cell needs.
This makes sense when you think about the biology - heart attack patients have a very different problem than most people admitted to the hospital (and different than all of those other groups in those unimpressive transfusion trials).
People having heart attacks have a mismatch between the blood supply that their heart needs and what it’s getting.
And the consequence of decreased blood supply to the heart is bad - worsening heart damage, which then brings on worsening heart function and less oxygen delivery, which worsens heart damage.
There’s the potential for a vicious snowball effect in patients with heart attacks that don’t have the oxygen carrying capacity that they need - and maybe, just maybe, this group of patients will benefit from more liberal blood transfusions.
As you can guess from the buildup, MINT was a positive trial - the first trial suggesting that more may be better when it comes to transfusions
The results in MINT were really interesting - transfusing to a higher threshold seems like it has a benefit:
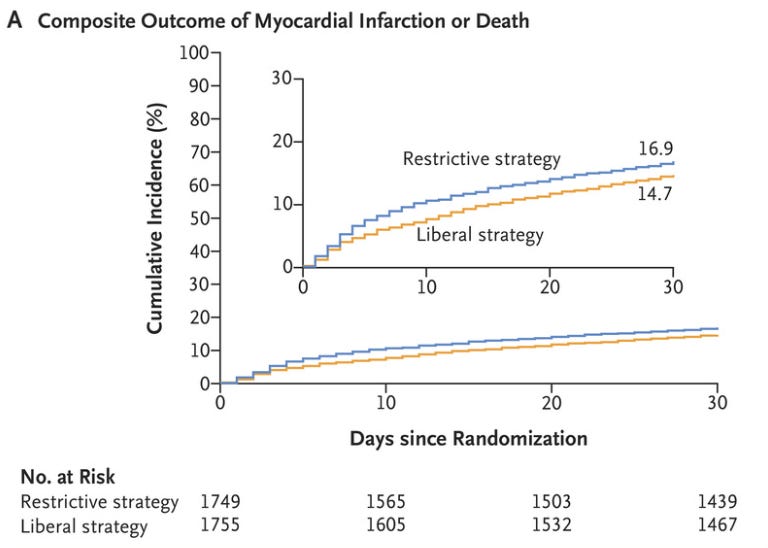
The benefit wasn’t technically statistically significant, but the confidence interval is 1.00-1.35. This means that the most pessimistic read is that more transfusions are the same as fewer, with a very high likelihood that there’s actually a benefit:

Color me surprised.
And when you look a bit deeper, you see that there was a pretty big difference in number of transfusions between the groups:

So it seems I was wrong in what I expected the trial to show - when it comes to patients with heart attacks, I think that more liberal blood transfusions is probably better.
The takeaway here isn’t to transfuse everyone equally - it’s to apply the results to the patient in front of you as an individual
Is the right conclusion to draw from MINT that every patient coming in with anemia and a heart attack should get a transfusion?
Absolutely not - and please don’t start having the same transfusion goal for every single heart attack patient.
The point I’ll take from MINT is that there’s a subgroup of people having heart attacks for whom anemia is a major problem that makes the heart attack worse.
Their low oxygen carrying capacity worsens ischemia to the heart, which makes the heart work harder, further increasing oxygen demand and making everything worse.
MINT will push me on the margins to think about which of my heart attack patients are sicker because of their anemia specifically worsening their heart’s oxygen supply/demand mismatch.
These patients - like many patients - will identify themselves with clinical signs or symptoms. I’m thinking things like ongoing chest pain or shortness of breath, rising markers of cardiac damage, worsening vital signs.
Those are the people that should have higher transfusion goals.
In the setting of a mixed bag of trials, it often means that there’s a subgroup of patients that benefits and the job of a doctor is to zero in on those folks as precisely as possible.
And so back to the question I led with: why was I wrong here?
Mostly because I hadn’t spent much time thinking critically about an issue I thought was settled - I thought we had enough data and that this was settled science.
The term for this cognitive bias is premature closure. And so I’m thankful to the MINT investigators for doing this trial.
I’ve learned a lot from this, and my patients will be better for it.