




You would think that answering a question like “does marijuana cause heart disease?” would be pretty easy to do.
Or that we’d at least have a pretty good answer to that question in 2024.
But it turns out that we don’t understand this relationship nearly as well as we should, given the massive experiment that much of the country is currently experiencing with rapid marijuana legalization and commercialization.
I get questions about this from patients all the time, including after a recent study published in the Journal of the American Heart Association got a lot of press.
The headlines seem to suggest that marijuana is bad when it comes to heart disease.
Here’s the New York Times:

Here’s CNN:

But after reading the paper, which you can find here, I’m not sold that we know anything different now than we did before this paper came out.
Why might marijuana impact heart disease?
Part of the Bradford Hill Criteria to ascertain causality from observational data requires plausibility - AKA a possible mechanism of connection.
So ever paper you read on marijuana and heart disease is going to include a bit about possible mechanistic links.
In the case of marijuana, you can think about risk as existing in two forms:
Risk related to the active ingredients in marijuana itself - i.e. does ingesting THC cause heart disease?
Risk related to the method of consumption - i.e. does smoking marijuana cause heart disease?
In the case of risk related to THC, the plausible mechanism is that there are cannabinoid receptors throughout the cardiovascular system and that THC has been shown to have a direct impact on raising blood pressure and heart rate, which may influence heart disease risk.1
The much more concerning link is really related to the mechanism of consumption. There’s data linking marijuana smoking to inhalation of particulate matter similar in nature to tobacco smoke. There’s also animal data suggesting that marijuana smoke worsens markers of cardiovascular function.
Sorting out risk 1 from risk 2 is really tough to do, and this study isn’t trying to answer that question.
This new study is the biggest study on marijuana and heart disease that we’ve ever seen
This study had a straightforward design.
The researchers took data from a survey run by the CDC, called the Behavioral Risk Factor Surveillance System, and assessed participants across 27 states and 2 territories from the period of 2016 to 2020 who answered the question “During the past 30 days, on how many days did you use marijuana or hashish?”
This survey evaluated presence of heart disease in a simple way - they asked people if they had heart disease:
Outcomes were assessed when respondents were asked, “Has a doctor, nurse, or other health professional ever told you that you had any of the following….?”. Coronary heart disease (CHD) was assessed by: “(Ever told) you had angina or coronary heart disease?” The lifetime occurrence of myocardial infarction (MI): “(Ever told) you had a heart attack, also called a myocardial infarction?” Stroke: “(Ever told) you had a stroke?” Finally, we created composite indicator for cardiovascular disease, which included any CHD, MI, or stroke.
They did statistical analyses to adjust for a few possible confounding variables: age, sex, education level, alcohol, tobacco, body mass index, diabetes, and physical activity.
The tobacco adjustment is notable because there’s been an argument in the cardiology literature to suggest that most of the risk of marijuana use is actually related to concomitant tobacco use - this paper tries to separate out the two.
What did these researchers find?
They found demographic information similar to what you expect: daily marijuana smokers are younger, more likely to be male, smoke more, drink more, and have less education than people who don’t smoke daily.
The researchers adjusted for those variables in their analysis, so you don’t need to be all that worried about what those differences mean.
After adjusting for all of the variables I described above, marijuana users had a 28% high risk of heart disease than non-users.
It’s interesting to see that there appears to be a dose-response relationship, with more frequent marijuana use being linked to a higher risk of cardiovascular disease:
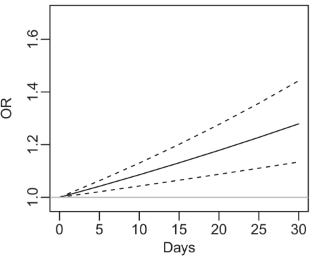
In the graphic above, OR means odds ratio - it’s basically a relative incidence of heart disease between days of marijuana use over a 30 day period compared to non-users. So a daily marijuana user has that 28% higher risk because their odds ratio is 1.28.
The dotted lines are 95% confidence intervals, which means that there’s a 95% chance that the result is between those dotted lines.
That gradation in risk related to exposure is another one of those Bradford Hill Criteria.
The reason I keep mentioning those criteria is that a study like this cannot prove causality because of its design, so we need to use methods to infer the likelihood that there is a causal relationship.
My top line on the results - this is a pretty underwhelming study that should change nothing for you
As I’ve already mentioned, this is an observational trial, so you simply can’t draw any conclusions about whether marijuana use causes heart disease based on a paper like this.
But I’m particularly unimpressed with these results in terms of how they will change my priors, for a few reasons.
First, the size of the association isn’t all that big. A 28% increase in self reported heart disease from using marijuana daily is less than I would have expected it to be if marijuana itself was truly a big deal in terms of cardiovascular risk.
Second, we can’t tease out the method of marijuana delivery from this trial. Lumping edibles with vaping with inhaling a burning plant is too heterogeneous a group for us to learn anything about the true impact of cannabis versus the method of consumption.
Third, they didn’t adjust for important confounders that might have made the association more persuasive. For example, hypertension wasn’t reported in the study.
But the most important reason that I’m not impressed is that you can’t adjust for every single variable here.
Do you really believe that the only difference between a 45 year old white man with a college degree and no diabetes who uses marijuana daily compared to another 45 year old white man with a college degree and no diabetes who never uses marijuana is the weed?
There are a million other things different about those two people that no demographic data is ever going to tease out.
If you haven’t heard the term healthy user bias, please clink on that link and familiarize yourself with it.
You can’t understand why this type of research is so unimportant without understanding that concept.
There are really important differences between people who are health conscious and people who aren’t that you can’t capture with survey data and that no epidemiologic study will ever be able to tease out.
And so I think we can just throw these results out with basically ever study you’ve heard about on coffee, nuts, or whatever else makes the news based on this type of research.
What do I tell my patients about marijuana?
As I mentioned earlier, patients ask about this stuff all the time, so I have a few thoughts that I make sure to touch on.2
We probably won’t ever know the direct impact of marijuana on heart disease
I doubt that regular use will lower your risk of a heart attack
It’s plausible to me that heavy use increases cardiovascular disease risk by a modest amount, but I would be surprised if it were on the order of magnitude of having diabetes or smoking a pack of cigarettes a day
Inhaling material that’s burning isn’t good for heart health, and it probably doesn’t matter much if that smoke comes from tobacco, cannabis, wood, or something else
If you are going to consume it, I feel comfortable that edibles are the safest method of ingestion
Vaping is probably better than smoking, although we don’t know what other ingredients may be present that can influence risk
I think a harm reduction framework is the best way for a physician to approach a topic like this. If my patients use edibles instead of smoking, I think that’s probably a win.
The dose makes the poison and if using a “safer” consumption method to increase overall consumption, that is probably bad.
So ultimately, I think it’s probably not good for your health to use marijuana regularly, but I don’t think it’s fair to say that a study like this suggests that even a small amount of marijuana use increases your risk of heart disease in a clinically significant way.
But before you take that and draw any conclusions, I want to point out that exercise also has a direct impact on raising blood pressure and heart rate, so that short term impact doesn’t necessarily mean anything about a long term impact either positively or negatively. After all, cocaine also raises heart rate and blood pressure, and I don’t think that anyone reasonable would argue that either exercise is bad for your cardiovascular risk or that cocaine is good for it.
I’m not an expert on the impact of cannabis on mental health, sleep, exercise, chronic pain, arthritis, or anything else - so I don’t bring up those aspects of health. I don’t keep expand the scope of my discussions with my patients because I don’t believe they’re seeing me for my loosely held and minimally-considered positions on any of the other things that cannabis might do for humans