


In defense of stress tests

A couple of weeks ago, I wrote an argument about why stress tests are overused and occasionally pointless:

The crux of that argument boils down to a straightforward thought experiment:
Abnormal stress tests frequently lead to a cardiac catheterization and a stent being placed
The evidence that putting stents in people who are not having heart attacks is any better than just treating heart disease with medicines is pretty limited
A stress test doesn’t tell you if somebody has early heart disease that isn’t causing a severe blockage in blood flow (and most blockages aren’t)
Therefore, it makes more sense to do an anatomic test like a coronary CTA to directly visualize the arteries around someone’s heart. This way, you can make an actual diagnosis of heart disease and then you can medically treat it
I think that argument makes logical sense, but I also don’t think it’s entirely right.
So, it’s time for me to argue with myself: let’s make the case for stress tests.

Stress tests give you more information than just whether someone has a severe blockage in an artery
While determining whether someone does or does not have a severe blockage in an artery is often the big picture goal of a stress test, that’s not the only thing you learn.
When you do a stress test, you don’t just get an answer about whether it’s positive or negative.
That’s often how it’s portrayed, or, as patients sometimes say, “I passed my stress test.”
In reality, however, there’s a huge amount of nuance to interpreting the result of a stress test, and a lot that you can learn about someone
Exercise capacity
During exercise portion of the test, you got to see what happens when somebody does physical activity as well as how much they can do.
You learn about the exercise capacity in an objective, validated, and quantifiable manner.
This is often much better than relying on a patient report of what their physical activity is. People often mislead their doctors, but even more often, they mislead themselves.
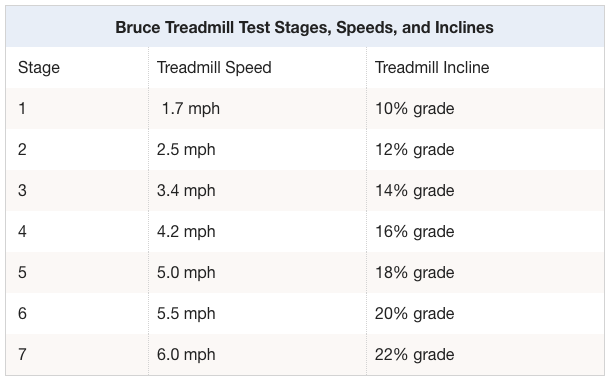
I can’t tell you how many people I have heard describe to me that they’re quite active and they never have a limit to what they’re capable of doing, but then when I put them on a treadmill, they’re only able to complete three minutes of exercise on the Bruce protocol.
So that we all have a shared mental model about what that means, here’s a chart. You spend 3 minutes at each stage of the test:
A person’s exercise capacity often changes the way you treat them medically, as the data are pretty clear that the higher your exercise capacity, the lower your likelihood of dying:

Poor exercise capacity may make me more likely to treat high blood pressure or high cholesterol with medications, and it certainly makes me more likely to counsel a patient on the importance of additional physical activity.
Whether someone is a reliable narrator of their own exercise capacity will also sometimes alter my impression of the reliability of the rest of the information they provide about symptoms.
You don’t get anything about exercise capacity from a CT scan, but you do get it from a stress test.
Prognostication
The data are pretty clear - almost every single variable measured in a stress test gives you information about your prognosis. Here’s a non-exhaustive list:
Ability to achieve target heart rate (85% of maximum predicted, which is 220 - age)
Heart rate recovery after exercise
EKG response during exercise
Blood pressure response during exercise
Irregular heartbeats during the test
Number and severity of abnormalities on the imaging portion of the test
The most common method of determining prognosis is the Duke Treadmill Score, but any of the pieces of information above give you important information.
Reproducing symptoms
The purpose of any medical intervention is to either make a patient live longer or feel better.
But in order to make someone feel better, you need to understand precisely why they don’t feel well.
And that brings us to the biggest issue with a CTA: just looking at somebody’s coronary anatomy doesn’t actually tell you if the symptoms that they’re having are related to blockages in the blood flow to the heart.
When somebody comes to see me with shortness of breath, if I just send them for a CTA, and I see that they have coronary artery disease, can we really be all that confident that the blockage that we visualized on the CT scan is the cause of their symptoms?
The answer is that we can’t. We can make an educated guess, but our level of confidence in that guess is not always going to be incredibly high.
With a stress test, when somebody is able to exercise, you can potentially reproduce symptoms.
If reproducing a patient’s symptoms goes along with an abnormality in blood flow visualized on the stress test, now we feel more confident that we understand what’s going on.
You can have chest pain without severe blockages seen on a CTA: the cautionary tale of INOCA
INOCA is an acronym that stands for ischemia with non-obstructive coronary arteries.
INOCA is an increasingly recognized reason that people have symptoms related to cardiovascular disease, but don’t actually have severe blockages in the major arteries around the heart when visualized on a catheterization or CTA.
This is a somewhat rare entity, but it isn’t a total zebra. In the ISCHEMIA trial, 13% of patients with markedly abnormal stress tests did not have severe blockages in the arteries around the heart when CTAs were performed.
That’s a pretty big collection of people who will be given an incorrect report that symptoms that they are experiencing are unrelated to heart disease.
And since this diagnosis is often missed, many people with INOCA have poor experiences with the medical system - lower quality of life, inaccurate diagnosis, symptoms blown off, and often quite a bit of suffering without an explanation.
INOCA has a few mechanisms, such as endothelial dysfunction or spasm of the small arteries or big arteries, but if all you do is a CTA and you skip the stress test, you’ll probably miss this diagnosis.
A stress test can help to answer important clinical questions here.
CTAs and stress tests are complementary, not competitive
Ultimately, the goal of everything that your doctor does should be to improve either the quality or length of your life.
Stress testing can often help us be more precise about the cause of someone’s symptoms and provide a quicker path forward to improving quality of life.
I view anatomical testing (like CT scans or catheterizations) to be complements to functional testing (like stress tests) rather than competitors.
And while this may feel like just another cardiologist advocating over-testing and over-medicalizing, that’s hopefully not what I’m doing.
I’m not advocating the indiscriminate use of testing, and I’m certainly not recommending anything about any type of testing for any specific patient. That’s the conversation you have with your own doctor.
When it comes to understanding why somebody doesn’t feel well, it’s important to provide an answer and also to help figure out the right treatment.
Different tests each provide a different utility, and there are often times when I order both a CTA and an exercise stress test when I’m evaluating a person who has symptoms suggestive of heart disease.