



If you’ve been reading this newsletter for a while, you know that I’m obsessed with polypills.
A polypill is a single pill that has a few different medicines in it. Poly comes from the Greek word for “many” and pill is self explanatory.
I don’t think it’s hyperbolic to say that on a population/public health level, it’s simply the best tool that exists for cardiovascular disease prevention.
I’m not the first one to raise this suggestion. By some estimates, if everyone over 55 took a polypill, about 80% of cardiovascular disease could be prevented.
There’s really compelling data that giving a specific type of polypill called Polycap lowers the risk of cardiovascular disease in people who have never had heart attacks or strokes:
And polypills also seem to be effective in populations with challenges in the social determinants of health, which is further reason to be excited about their potential benefit across society.
And we have intriguing new data in patients after heart attacks further bolstering the case for polypills.
A new study on polypills for people who already have heart disease - more data, but some unanswered questions
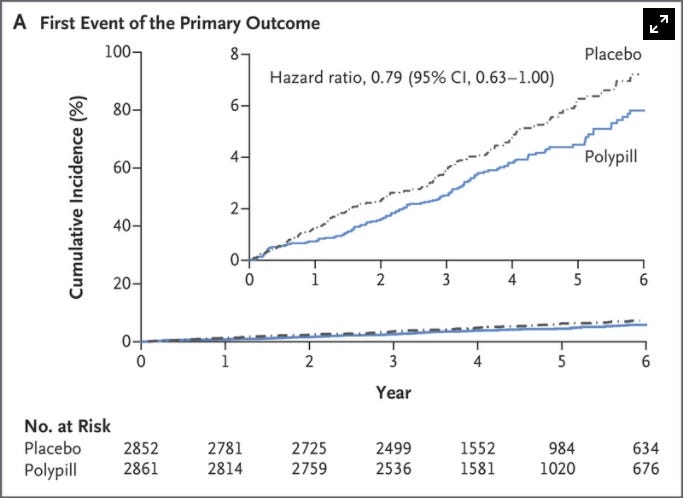
Data from the SECURE trial was just presented at the annual European Society of Cardiology meeting.
This was a study looking at people who had a heart attack in the last 6 months and either giving them a polypill or “usual care.”
The polypill in this study was composed of 3 different drugs:
Aspirin 100mg dose - a blood thinner
Ramipril either 2.5mg, 5mg, or 10mg dose - an ACE inhibitor (lowers blood pressure and has some cardioprotective effects)
Atorvastatin either 20mg or 40mg dose - a statin (lowers lipids and reduces heart disease risk)
The people in the usual care group were able to get any of the medications that were in the polypill. And the polypill group could also take additional medications.
It shouldn’t be surprising that polypills look great in the SECURE trial, just as they have in the other trials that they’ve been studied.
Just look at the curves showing event rate over time:

Patients in the polypill group reported better adherence to their medication (and that’s hypothesized to be why they had such an impressive reduction in risk).
But here’s the weird part - the people in the polypill group had better cardiovascular outcomes despite the fact that risk factor control was identical.
I mean, look at this chart from the supplementary appendix. The patients in the polypill group had identical blood pressure and cholesterol numbers to the usual care group:

I’m not totally sure what to make of this finding. What’s the mechanism of action here? The authors of the study (and accompanying editorial) make some hand-wavy guesses, but it’s a perplexing result.
This surprising piece of data doesn’t ultimately make me doubt the polypill as a concept - after all, if events went down, that’s what we care about.
Who really cares what your cholesterol numbers look like if you have a heart attack?
The SECURE trial provides additional evidence to support the fact that polypills prevent heart disease
Should you be taking a polypill?
I don’t think that there’s something magical about the idea of putting a bunch of medications all together.
In other words, if you have high blood pressure, an abnormal lipid panel, and high blood sugar, you don’t automatically do better just because all of your medications can be swallowed with one sip of water.
Risk factor control is risk factor control. And I think what a polypill does best is that it targets multiple different things that cause heart disease simultaneously, and that control leads to a synergistic benefit that increases over time.
So if you’re doing really well on the medicines that you’re taking (or if your medications are already sorted for you to simply adherence with a service like PillPack), it’s probably a stretch to make the argument that you’ll do better with a polypill.
But the majority of us would likely do better with a simpler approach.
Most people miss doses of medicines. They forget to pick up a refill before they run out. They have a medicine that’s prescribed twice a day that they only take once a day. Or any one of the million other reasons why medical treatments are tough to follow.
The magic of a polypill lies in the ease of implementation.
While I love the intellectual challenge of personalizing medicine and optimizing each individual patient’s unique risk factors, most of us would probably do better with a “set it and forget it” approach.
It’s a shame that polypills aren’t available commercially in the United States.
I find the argument that everyone over the age of 55 (and you could even convince me of younger) should be taking a polypill to be incredibly persuasive.
Here’s what I would put in a polypill
I don’t think that the polypills that have been studied so far are close to the optimal medications.
The Polycap pill, in particular, has suboptimal medicines in in, including simvastatin and atenolol (superior alternatives to both of these medications exist).
Here’s what I would put in my dream polypill for cardiovascular disease prevention:
Rosuvastatin - a statin
Telmisartan - an angiotensin receptor blocker (ARB)
Aspirin - a blood thinner
Dapagliflozin - an SGLT2 inhibitor
Let me explain why in detail.
Rosuvastatin
The evidence for statins in cardiovascular disease prevention is really strong, even if lots of people on the internet try to convince you otherwise.
Rosuvastatin (Crestor) and atorvastatin (Lipitor) have the most robust evidence base behind them, and they’re also the most potent. I also use pitavastatin and pravastatin in my practice, but I use them both less than the other two.
I favor rosuvastatin for a few reasons.
First, my patients seem to tolerate it really well, with a super low incidence of side effects. Second, it’s probably the most potent at risk reduction of all the statins.
Third, it is hydrophilic, rather than lipophilic. There’s controversy about the clinical difference (if there even is one) between lipophilic and hydrophilic statins. But some people suspect that the lipophilic statins, which cross the blood brain barrier more easily, may have a higher incidence of cognitive side effects.
While I think atorvastatin is a great drug, and I prescribe it quite a bit, I think rosuvastatin is just a tiny bit better, so that’s why it’s in my polypill.
Telmisartan
This is a type of medicine called an angiotensin receptor blocker (ARB). ARBs are the cousins of ACE inhibitors, both of which are commonly prescribed blood pressure medicines that also improve the ability of our blood vessels to dilate (medical term: improved endothelial function).
You could probably substitute telmisartan with any medicine in the same or similar class - really, any ARB or ACE inhibitor would do almost identically here.
I chose telmisartan in particular for two reasons:
ARBs are better tolerated than ACE inhibitors, which cause a dry cough in about 10% of people who take them. There’s a compelling argument that we should be using ARBs as first line treatment all the time over ACE inhibitors
Telmisartan may improve metabolic parameters more than other ARBs. There’s some data to suggest that telmisartan improves insulin sensitivity.
Aspirin
This is a controversial decision.
I’ve written about the controversy surrounding aspirin before in this newsletter.
The quick and dirty summary about aspirin is that it prevents heart attacks and strokes but increases the risk of bleeding.
For most people who have never had a heart attack or stroke, the risk is about equal in magnitude to the benefit.
So I would feel comfortable offering a polypill in a version with aspirin and a version without.
Dapagliflozin
This is my favorite medication on the list.
Dapagliflozin is in a class of medicine called SGLT2 inhibitors.
Originally developed as a medication to treat diabetes, we’ve subsequently learned that these medicines help patients with heart failure, kidney disease, and, yes, diabetes.
There’s even evidence that these medications extend lifespan in mice.
I am of the belief that it’s only a matter of time before these drugs become considered an important part of the general prevention of cardiovascular disease, which is getting increasing attention in academic circles.
While I briefly touched on SGLT2 inhibitors in this newsletter more than a year ago, I haven’t given them the attention that they deserve. I’ll be diving into SGLT2i’s in more detail in their own newsletter sometime soon.
So, in summary: polypills are fantastic, and we haven’t even come close to optimizing them yet
In some ways, the future of medicine is already here.
We know a huge amount about how to prevent cardiovascular disease, and it isn’t a mystery. Have lifelong control of blood pressure, blood sugar, and cholesterol. Don’t smoke. Get regular exercise. Reduce stress. Have purpose. Maintain social connections.
A polypill strategy gets most of us most of the way there. And we should be using this approach much more.
Thank you for reading and subscribing! Please share freely with friends and family and encourage them to subscribe!