
What Should You Do With An Abnormal Stress Test?

Today’s newsletter is about a patient of mine.
He’s a 65-year-old man who came to see me because of chest pressure that started 30 minutes into his workouts on the elliptical. The symptoms had been going on for a few months and hadn’t really gotten worse. He’s been relatively healthy. He has mildly elevated LDL, well-controlled hypertension on one medication, no diabetes, no smoking, no significant family history. Not a particularly high-risk patient.
His primary care doctor wasn’t particularly alarmed by the symptoms. But he ordered a coronary calcium score, reasoning that it would be the easiest and cheapest way to rule out a cardiac problem. The score came back at 187. The patient freaked out and his doctor sent him to me.
Before I tell you what happened next, I need to make a brief but important detour.
Aside: a coronary calcium score has zero role in the evaluation of chest pain
I want to say that clearly because I see this mistake made all the time.
A calcium score doesn’t tell you anything about whether there’s an obstructive blockage. You can have a calcium score of 1500 and have no significant narrowing anywhere in your arteries. You can have a calcium score of zero and have a massively obstructive plaque (the high risk, might rupture and cause a heart attack kind) sitting in a large artery.
The calcium score tells you about the burden of calcified plaque, not the degree of stenosis.
If you’re ordering an imaging test to evaluate a symptom someone is having, the test you want is a coronary CTA. (And while we’re here, I don’t think AI-powered assessments add much to the coronary CTA either, but I’ve written about that separately.)1
Another quick aside on evaluating chest pain before we get back to our patient
When he came to see me, what immediately got my attention was the pattern of his symptoms.
The single most important question I’m asking when I evaluate chest pain (or almost any symptom a patient reports) is whether it’s exertional or not.2
Something that happens at rest is less likely to be cardiac. Something that happens with exertion is more likely to be cardiac.
After that, I’m paying close attention to duration: a symptom that lasts a few seconds probably isn’t cardiac; a symptom that’s been continuous for days without resolving is also probably not cardiac. Classic cardiac chest pain comes on with exertion and resolves after a few minutes of rest.
That’s not a perfect heuristic, but it gets you pretty far.
I’ll add one more thing here, because it comes up often: a patient doesn’t need to have chest pain or pressure to have a blocked artery. Women are sometimes described as having “atypical symptoms,” as if crushing chest pressure is the standard against which everyone else is measured. It’s accurate that women are less likely to have classic chest pain with a heart attack, but my experience is also that anyone can present without classic symptoms.
I pay far less attention to the character of the discomfort than I do to its pattern. And this patient’s pattern was textbook. Exertional pressure at the end of a workout, resolving with rest.
It’s concerning.
To evaluate his symptoms, I sent him for a stress test
The next step I took was to order a stress echocardiogram. A stress test here serves two purposes for me: 1) it helps me make the diagnosis more clearly, and 2) gives me prognostic information.
My patient’s test was markedly positive. He had ECG changes on the treadmill, and the anterior wall of his heart showed reduced motion when his heart rate was elevated.
Both of those findings point toward significant blockage in the LAD territory.
But here’s the part that matters just as much as the positive result: he went 10 minutes on the Bruce protocol.3
Ten minutes is a pretty impressive exercise capacity for a 65-year-old man.
And exercise capacity on a stress test is one of the most powerful prognostic variables we have. It’s arguably more important than most of the other data you get on a stress test.4
A patient who can go 10 minutes on the Bruce is telling you something important about their overall cardiovascular risk.
So what should we make of these two discordant pieces of information?
The stress test is clearly pretty abnormal - the degree of ischemia meets the ISCHEMIA trial’s definition of “moderate” - but his exercise capacity is reassuring.
A stress test isn’t a binary normal vs abnormal. It’s a result on a continuum, and you have to interpret all the data, not just the top line report.
What I did next
The stress test result made me feel pretty confident that my patient had a severe blockage in his LAD.
And after that result, I had 2 major items on my agenda.
First, I took a careful history to ensure that his symptoms were stable.
This distinction matters a ton. Classic chest pain that’s been unchanged for months is stable. But if the pattern has shifted and symptoms are coming on earlier in exertion, or at lower workload, that suggests something is changing.
And the key point here is that it’s not about the severity of the pain. A 2/10 chest pressure that’s now coming on at the start of the workout is more worrying than an 8/10 that’s still happening at the same point in the same workout.
Earlier onset at lower exertion suggests an unstable process, which is generally treated as a medical emergency.
Thankfully, his symptoms were totally stable.
Second, I started him on medication: a high-intensity statin, a beta blocker, and aspirin (I’ll acknowledge the aspirin is a judgment call in stable disease, but at the time I viewed it as likely temporary while we figured out next steps).
With the beta blocker on board, his symptoms improved. He was completing his workouts without chest pressure.
After that, I ordered a coronary CTA (both because it’s embedded in the ISCHEMIA trial protocol, and because I think anatomy matters when you’re making a shared decision about what comes next).
On the CTA, we’re looking to understand his total burden of disease and define his anatomy. There’s a world where he actually has so many blockages in so many arteries that we might have to discuss bypass surgery.
His CTA showed single vessel disease, a severe stenosis in the mid-LAD, which mapped identically to his stress test findings.
You need to know the ISCHEMIA trial to make the next set of decisions
I think we now have a complete picture about what’s going on.
My patient has stable angina from single vessel coronary artery disease. His symptoms are controlled on a low-dose beta blocker. His risk factors are well-managed. He can walk 10 minutes on the Bruce protocol.
So what do you do?
This is exactly where the ISCHEMIA trial becomes one of the most important pieces of evidence I practice with.

ISCHEMIA enrolled patients who look a lot like this patient: stable coronary artery disease with a markedly abnormal stress test and a coronary CTA confirming the anatomy wasn’t surgical (no left main disease, no anatomy requiring bypass).
The trial randomized patients to an early invasive strategy (cath lab, stents) versus a conservative strategy (optimal medical therapy, with catheterization reserved for cases where medical management fails).
It’s worth emphasizing how abnormal the stress tests were in ISCHEMIA. These weren’t borderline positive tests. These were the kinds of results that require the reading cardiologist to call the referring physician before the patient goes home.
Truly abnormal. Most abnormal stress tests in the real world don’t come anywhere close to the threshold required for trial enrollment. That point matters when you’re trying to apply the evidence to practice.
The headline result from ISCHEMIA: an early invasive strategy did not provide a survival benefit compared to optimal medical therapy
But the data are more nuanced than the headline suggests, and that’s actually what makes ISCHEMIA so interesting.
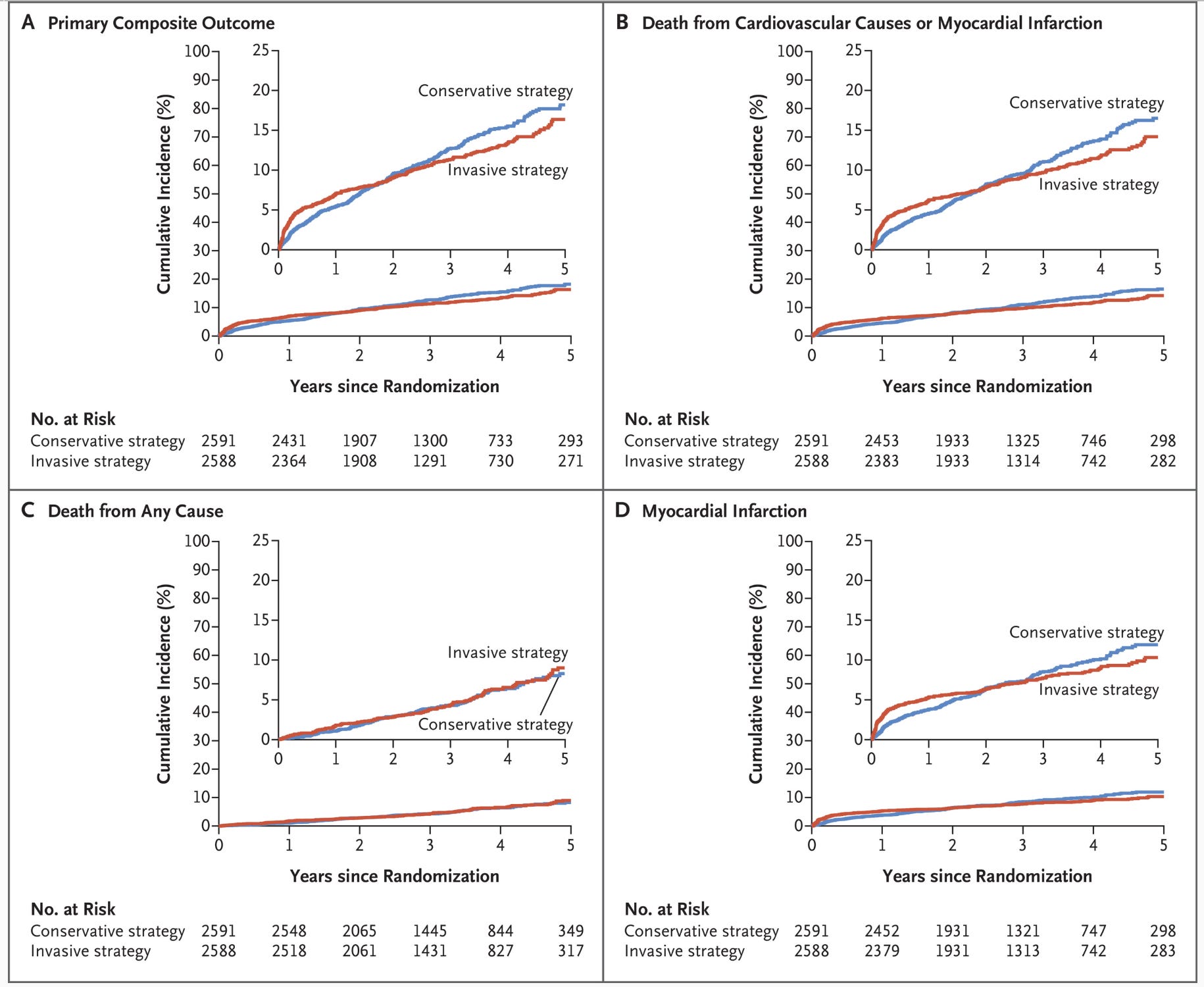
There’s something in it for everyone. If you read carefully, the invasive arm had an early procedural risk (because anything invasive carries risk) but appeared to prevent myocardial infarctions when you follow the patients long enough:5
When you talk to Judy Hochman, ISCHEMIA’s principal investigator, about what she’d want clinicians to take away from the trial, her perspective is worth hearing:
Dr. Hochman’s main message is shared decision making. Both approaches are valid. The conversation about what fits with a patient’s preferences and their risk tolerance is the most important thing to consider when making a decision about which strategy to choose. This shouldn’t be a rushed discussion at the end of a busy clinic visit where the default is whatever the referring doctor already had in mind.
One more thing that gets underweighted in how people talk about this data: it’s not an emergency decision.
Even under the most optimistic reading of the invasive strategy reduction in heart attack risk, it takes years to show up.
There is no evidence that rushing someone with a markedly abnormal stress test to the cath lab the next morning improves their outcome. And yet that is often exactly what happens.
What my colleagues said about the case
This is the sort of case where different people often have different perspectives. And for this case, I asked about 8 of my colleagues what they would do if this was their patient.
Every single one of them - except Dr. Hochman, who said that we needed to do shared decision making - said they would go to the cath lab.
The reasoning was consistent. The blockage is clearly severe.6
When you put in a stent and fix the blockage, you’re no longer spending mental energy worrying about it every time you exercise. You’re not watching for symptoms. You’re not adjusting medications.
Several colleagues framed stenting as the lower-anxiety decision, not because it was medically necessary, but because it allowed them to stop wondering about what would happen next.
I don’t think that’s an unreasonable position. And if you look at the ORBITA trial, which randomized patients with stable angina and severe stenosis to stenting versus a placebo procedure, the patients in the medical management arm ended up on a fairly heavy medication burden to control their angina. That’s real.
What happened in this case
After a thorough conversation, we decided on a medical management first approach.
As with many clinical situations, eventually the patient tells you what the right answer is.
In this csae, his symptom relief didn’t last. A few months later, he developed more chest discomfort on the elliptical.
The symptoms were returning despite the medication, so we sent him to the cath lab.
He got a single stent placed without complication. Within a week he was back to exercising.
His exercise capacity - by his own report - was better than it had been before his symptoms started. He came off the beta blocker. He was happy.
But the alternative path would have been completely reasonable. Augment the medications, watch carefully for symptom progression, and revisit if needed.
The reason I find this case worth writing about is that it illustrates something I see a fair amount: the rush to do something invasive with an abnormal stress test.
The assumption that too many people make it is that a scary-looking stress test means you need to put a stent in right now.
ISCHEMIA tells us that we don’t need to force the trip to the cath lab instantly.
It doesn’t tell us that stents are bad. It tells us that for stable patients with even very abnormal stress tests, doing nothing invasive right away (as long as you are planning on medical therapy) is a legitimate and well-supported strategy.
The decision belongs to the patient, informed by a real conversation about what the evidence actually shows.
Coronary calcium scores remain useful for risk stratification in asymptomatic patients — the setting for which they were originally validated. They are not an appropriate substitute for functional or anatomic testing in the evaluation of symptoms.
To read more about my perspective on what your doctor is listening for when you’re describing symptoms, here’s my piece on why your doctor keeps interrupting you and how to fix it:

If you’re not familiar with the Bruce protocol, it’s the standard treadmill stress test. You start at 1.7 miles per hour at 10% incline and go for 3 minutes. Then every 3 minutes things get faster and more inclined. You go until the treadmill wins.
The relationship between exercise capacity and cardiovascular outcomes is really quite robust. I’ve written separately about how VO2 max as a marker is often misapplied in this context: Your VO2 Max Protocol Is Based on A House of Cards
The ISCHEMIA-CKD substudy, which enrolled patients with chronic kidney disease, did not show any heart attack benefit from the invasive strategy, a finding that adds nuance to how broadly we apply the main trial results.
The oculostenotic reflex is powerful.
Some of the most practical and well-articulated clinical reasoning for ASCVD risk stratification and management I've read. Thank you for writing this up.
Thank you for sharing this story with us! Such a high-value piece as it does something rare in public-facing cardiology writing: it shows that an “abnormal stress test” is not a command, but it’s the start of a more careful conversation. What really stands out is your insistence on pattern over panic. Exertional symptoms matter. Stability matters. Exercise capacity matters. Anatomy matters. And once you lay those pieces together, the decision becomes much more adult than the usual reflexive “positive test = cath lab tomorrow”.
I also appreciate how clearly you translate the ISCHEMIA lesson. Too many people hear “no immediate survival benefit” and conclude either that stents are overused or that medical therapy is somehow passive. Your case shows the more honest middle: for stable patients, time exists for shared decision-making, medication optimization is a real treatment strategy, and the patient’s symptom trajectory often tells you when the invasive path becomes the right one.
And honestly, your colleagues’ responses were revealing in the best way. The pull toward intervention is not always about evidence alone; sometimes it’s about uncertainty tolerance for doctors and patients alike. Naming that makes the whole discussion more trustworthy.