
What's up with HDL?

In many ways, the story about HDL1 is simple: in general, having a higher level seems to be protective against heart disease, but raising that level with medications doesn’t seem to be beneficial.
On a population level, that relationship seems straightforward - people who have higher HDL levels seem to have a lower risk of heart attacks and strokes.
When you start digging a little bit deeper, HDL starts to get more complicated:
Some people with extremely high levels of HDL cholesterol may have a higher risk of heart disease
But some genes linked to high HDL are common in people who live to over 100 and seem to provide protection against heart disease and Alzheimer’s2
Some genetic variants with low HDL levels seem protective against heart disease
Other genetic variants with low HDL seem to increase heart disease risk
It’s easy to read this stuff and feel like your head is spinning.
There’s clearly more to the HDL story than just what your numbers look like on the standard blood tests that we have.
We just don’t understand the biology of HDL well enough to manipulate it yet, but there are ongoing hypotheses about what might be happening.
And so I looked at a recent study presented at the ACC Conference and published in NEJM called AEGIS-II with great interest to further illuminate the HDL story.
HDL seems good, but it’s been useless as a treatment target so far
As I mentioned before, the history of HDL raising efforts have been pretty unimpressive.
There’s the saga of a class of drugs called CETP inhibitors, which raise HDL and lower LDL cholesterol:
Torcetrapib was studied in the ILLUMINATE trial, and was found to increase the risk of death even though it made lipid panels look amazing.3
Dalcetrapib was studied in dal-OUTCOMES, where it increased HDL but didn’t reduce heart disease.
Evacetrapib was studied in ACCELERATE, and just like dalcetrapib, was similarly unimpressive in its impact on heart disease even if the lipid panels looked better
Anacetrapib was studied in REVEAL, where it reduced heart disease risk proportional to LDL reduction, not HDL raising. The results were unimpressive enough that Merck didn’t file for FDA approval for the drug
Niacin is the other big part of this story. On the surface, addition of niacin makes people flushed but seems to improve their lipid panels.
Unfortunately, HPS2 THRIVE and AIM HIGH didn’t show that niacin reduces cardiac events.
Niacin also has the side effect of worsening insulin resistance and metabolic syndrome, and I don’t think it has any real role in the management of cardiovascular disease.
Since most experts are converging around the idea that HDL function is really what matters, clinical trials have turned their focus to function
One of the things that HDL does is participate in something called reverse cholesterol transport, which removes cholesterol from the walls of our arteries.
The first step in that process is something called cholesterol efflux. Improved cholesterol efflux capacity has been linked to a lower risk of heart disease.
Cholesterol efflux is mediated by the function of apolipoprotein A-1, which is the major apolipoprotein in HDL particles.4
And so that’s where AEGIS-II comes in - the investigators asked the question, “what if we don’t even try to raise someone’s HDL levels, but we just give them the functional stuff by infusing apolipoprotein A-1?”
AEGIS-II infused post heart attack patients with apolipoprotein A-1 to try to improve their cholesterol efflux and reduce their cardiac risk
This trial took patients with recent heart attacks and randomized them to weekly infusions of apolipoprotein A-1 or placebo infusions.
This type of infusion has previously been studied and shown to increase HDL levels and to augment cholesterol efflux capacity.
So if cholesterol efflux capacity plays a big role in reducing risk after a heart attack, a trial like this should be effective at testing that hypothesis.
They followed patients for 90 days, which is the length of time after a heart attack when the risk of another cardiac event is the highest.5
The results weren’t very impressive - no statistically significant reduction in heart attacks, strokes, and cardiovascular death:
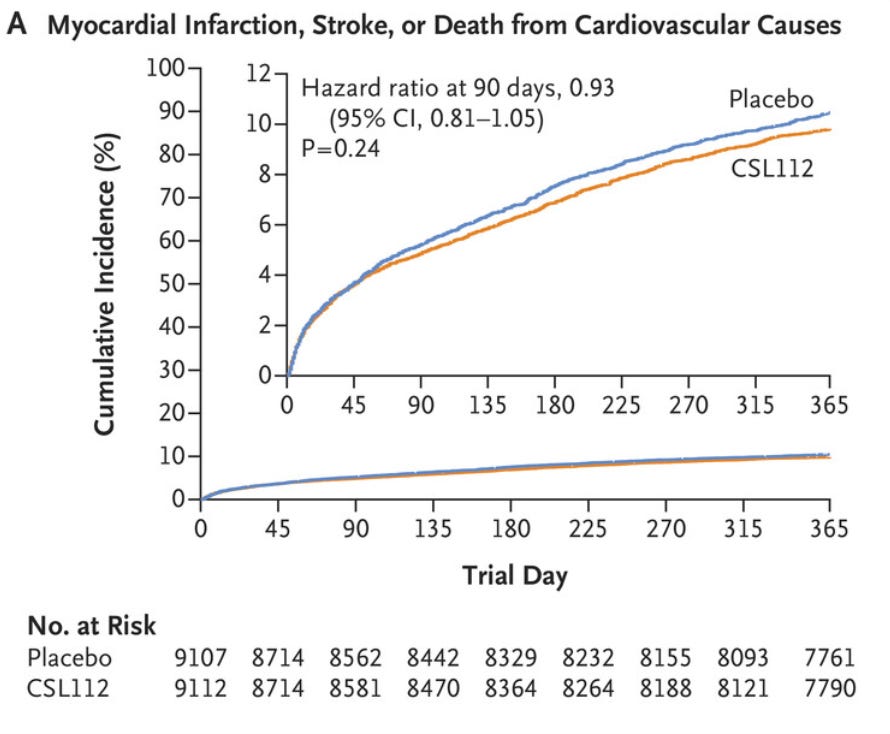
It’s a pretty unimpressive result, which fits with the body of the HDL literature.
What can we learn about HDL from a trial like this?
I think that’s a hard question to answer.
One possible explanation is that cholesterol efflux capacity is just a marker for people who are healthier, and that using it as a therapeutic target isn’t something that’s worth pursuing further.
I’m not there yet, for a few reasons.
One simple issue is that this trial didn’t assess cholesterol efflux capacity to identify people with poor capacity who would be most likely to benefit.
But the more important issue has to do with what HDL function is really doing - is it addressing risk of a heart attack or is it a driver of the pathophysiologic of cardiovascular disease.
I suspect that cholesterol efflux is a bigger deal in the long term process of plaque formation rather than something that’s making it’s primary impact on the risk of one of those plaques rupturing.
If poor HDL function is playing a causative role in atherosclerotic disease, I would expect treatment to be beneficial over a longer time frame as HDL modifies the long term process of atherosclerosis, rather than being a primary mediator of recurrent heart attacks in an unstable patient.
Another even more mundane possibility is that HDL function is important, it just isn’t *that* important for most people.
HDL remains a biologic conundrum and maybe the most accurate explanation is that we just need the basic science to catch up to what’s suggested based on the epidemiology.
For the purposes of this newsletter, when I write “HDL,” what I’m really referring to is HDL-cholesterol (often abbreviated HDL-C). The distinction here is important for people deep into the science. HDL refers to the lipoprotein particle, which is a combination of cholesterol, triglycerides, phosphoslipids, and apolipoprotein A-1. HDL-C refers to the amount of cholesterol carried by these particles. It’s not a measure of those particles or a marker of the quality of their function. These distinctions matter when you’re thinking about biological mechanisms, but they don’t matter much when you’re just talking about treating patients or interpreting your own lipid panel.
This is the gene for CETP, or cholesterol ester transfer protein, which is a fascinating story that I’m planning to write about in the future. A drug targeting this pathway is the single most exciting potential advancement on the horizon for the treatment of cardiovascular disease in my opinion
Torcetrapib has an off target effect of mimicking a hormone called aldosterone, which raised blood pressure and was probably responsible for the negative impact seen in this trial
Apolipoproteins come in many forms. You’ve probably read stuff in this newsletter on apolipoprotein B, the functional player in the particles that cause heart disease, like LDL, VLDL, and Lp(a)
If you look at Kaplan Meier curves from almost any post heart attack trial, they look very similar - risk increases fastest over the first 3 months and then tapers off.