
Why is Mounjaro better than Ozempic?


I think that the incretin mimetics are the biggest deal in healthcare today.
By incretin mimetics, I am referring to the weight loss drugs that are all over the place these days - Ozempic, Wegovy, Mounjaro, Rybelsus.
For today’s newsletter, I’m not going to belabor the same stuff that I’ve been talking about over and over again, but I will rehash it quickly:
These drugs work really well to promote weight loss
These drugs have excellent cardiovascular safety
When you start patients on low doses and increase slowly, these drugs are very well tolerated
When these drugs are used on the correctly selected patient, they cause people to lose predominantly fat rather than muscle
My read of the data is that tirzepatide (AKA Mounjaro) is a better drug than semaglutide (Ozempic).
For today’s newsletter, I wanted to explore why the story of other diseases tell us that this isn’t surprising as well as what it might mean about a new drug coming down the pipeline soon.
Treating complicated diseases often requires working on multiple biologic mechanisms
Pick almost any chronic disease that impacts a lot of people and causes significant morbidity and mortality.
When you look at treatments for that disease, you’ll see that the most effective treatments are often targeting multiple biologic pathways at the same time.
Congestive heart failure
The standard of care for treatment of chronic heart failure is to treat people with what is termed “Guideline Directed Medical Therapy,” or GDMT.
Most heart failure experts will tell you that the goal of treatment is to get people on quadruple therapy - 4 different drugs that all target slightly different biochemical pathways.
There’s a huge amount of literature on tackling the obstacles to getting people on all of the different classes of drugs, but the consensus is clear that targeting multiple physiologic pathways is the way to go.
HIV
HIV treatment has enabled a lot of patients with a new diagnosis to maintain a normal CD4 count and undetectable HIV viral load for many years, turning what used to be a death sentence into a chronic disease.
All of the contemporary HIV treatment strategies include multiple drugs, which makes sense to reduce the likelihood of creating resistance and obtain long term viral control.
Heart attacks
When someone has a heart attack, the first drug that everyone takes at home is an aspirin. Aspirin works to treat heart attacks because it inhibits platelets, a type of blood cell that causes blood clots to form.
But did you know that adding another drug that inhibits platelet activity (through a different mechanism than aspirin) improves heart attack outcomes on top of just aspirin alone.
This list goes on and on - you can talk about cholesterol lowering, pulmonary hypertension, hepatitis C, or tuberculosis.
Complicated diseases are often treated by attacking multiple biologic mechanisms at once, so why should obesity be any different?
Tirzepatide seems better than semaglutide
You can be really smart about this or you can be really simple.
The simple way is to look at the two trials investigating weight loss.
Tirzepatide (Mounjaro) leads to about 20% of body weight lost after a little bit over a year according to the SURMOUNT trial:

Semaglutide (Ozempic, Wegovy, Rybelsus) leads to about 15% of body weight lost after a bit over a year according to the STEP 1 trial:

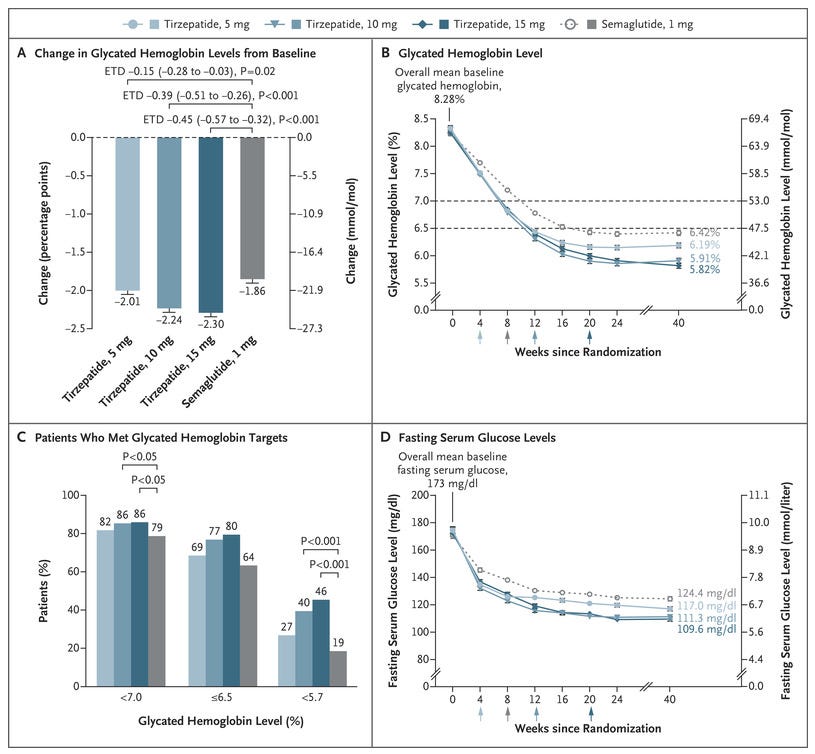
You can also look at a head to head comparison, the SURMOUNT-2 trial, which showed the tirzepatide was better than semaglutide at lowering blood sugar in diabetic patients:
And clinically, at least in my experience, tirzepatide is way better tolerated than semaglutide. Less nausea, less vomiting, less diarrhea, less constipation.
It seems to be that the drug is both more effective and better tolerated.
I’m not surprised because of the mechanism of action here.
Tirzepatide works on both major hormones of the incretin system - GIP and GLP-1. Semaglutide only works on GLP-1.
As we discussed above, inhibiting multiple pathways is often more effective than just inhibiting one pathway.
A drug to be really excited about in the future: retatrutide
The New England Journal of Medicine just published data on a phase 2 trial of retatrutide, which is a drug that stimulates GLP-1 and GIP (just like tirzepatide) but also stimulates another hormone called glucagon.
The term that’s being used for this drug is a “triple agonist” because it works on 3 different hormone receptors at once.
Retatrutide has a lot of promise when it comes to weight loss based on the phase 2 data, where a huge proportion of people achieve significant weight loss:

The addition of stimulating glucagon receptors makes some mechanistic sense to me, at least based on my understanding of semaglutide and tirzepatide.
The GIP and GLP-1 drugs mimic the incretin system - they are hormones released in the intestine in response to eating - so I’m not surprised that people taking these drugs report that their appetite is surpressed.
Glucagon is released in response to a protein rich meal, so retatrutide may just be stimulating an additional biochemical pathway that mimics the biological response to eating.
Be careful before jumping to conclusions here - the road to hell is paved with biologic plausibility
There are a million stories in medicine of a drug that “should” work based on our understanding of the biology that don’t work when randomized clinical trials are done.
We don’t understand biology perfectly, and it takes a lot of hubris to think that we do.
We don’t know what safety signals the phase 3 trials will reveal, and whenever you are looking at a new drug, the correct thing to do is be wary of the possibility of off target biologic effects that increase the risk of death.
One of the best examples of this is torcetrapib, a CETP inhibitor that was supposed to revolutionize the treatment of heart disease. The only problem is that it increased risk of death compared to placebo, probably because it raised blood pressure.
That said, it’s always worth going through the thought exercise of why something may be likely to be effective and then do the experiments to see whether it is.
The signal that working on multiple biological mechanisms is better than working on one is a common finding across many different areas of medicine, and it’s part of why I find the Mounjaro data so persuasive and part of why I’m excited to see the phase 3 results of retatrutide.
In the case of the revolution in weight loss drugs that we are currently living in, there is reason to be optimistic that the best is yet to come.