




Another study presented at ACC this past week asked the question “does Ozempic help to treat heart failure?”1
Heart failure comes in a lot of different types - not every patient with this diagnosis is the same.
The type of heart failure that this study investigated was heart failure with a preserved ejection fraction, also known as HFpEF, which is notoriously difficult to treat.2
The history of clinical trials in HFpEF is littered with failed drugs that seemed promising until clinical trials didn’t show much evidence of benefit.
The STEP-HFpEF DM trial comes a few months after the STEP-HFpEF trial suggested the possibility of a large benefit of Ozempic in these patients.3
STEP-HFpEF DM showed a benefit in measures of quality of life in diabetic patients with HFpEF
This trial looked at patients with HFpEF and randomized them to escalating doses of Ozempic compared to placebo.
They measured their weight over the year of the study and evaluated efficacy of the drug based on how patients answered questions on something called the Kansas City Cardiomoypathy Questionnaire, which is a validated tool in assessment of quality of life in heart failure.
The KCCQ asks questions about how frequently your quality of life has been impacted by heart failure over the last two weeks. Here’s 2 of the 8 questions:

It’s important to think about the endpoint in a trial like this.
Studying a drug that you’re going to give to a group of pretty sick patients usually requires demonstrating a benefit in more medicalized areas: heart attacks, strokes, death, hospitalizations for heart failure, etc.
And so it’s certainly interesting to see a study looking at quality of life metrics alone,4 but we’re probably going to need to see a longer trial looking at some of those other outcomes before this becomes widely prescribed in heart failure patients, who are already often on a lot of other medications.
The results here are unsurprising: losing weight makes quality of life better
It shouldn’t be surprising that a drug that helps people lose weight also improves their answers to questions on things like shortness of breath and fatigue.
Unsurprisingly, Ozempic improved both outcomes - patients lost weight and they reported improved quality of life:
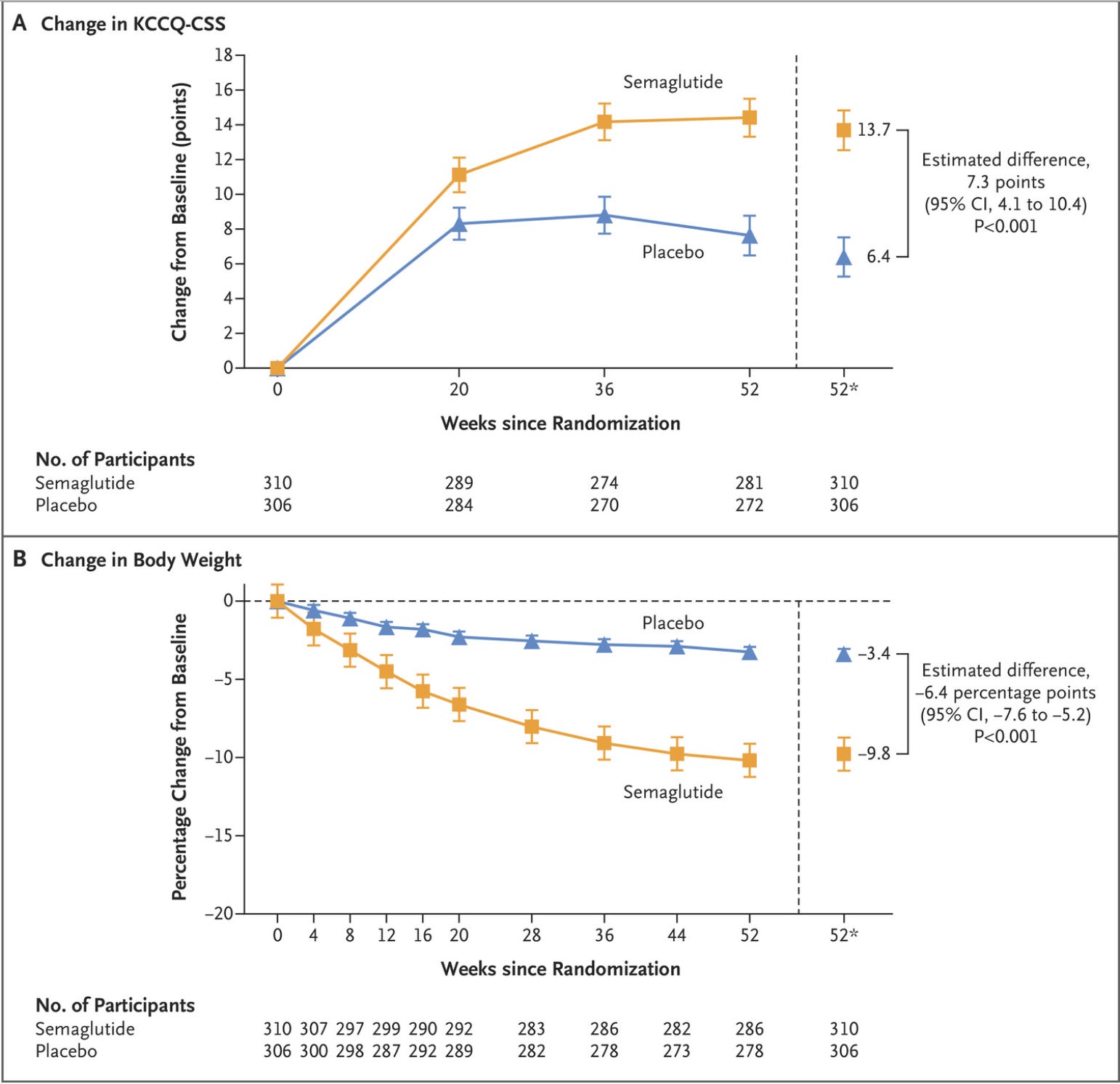
The impact of the drug persisted out to a year and, to some extent, corresponds to the amount of weight that was lost.
There are a couple of possible takeaways from this trial
I think you can look at these results and draw conclusions in 3 major buckets:
Ozempic is a weight loss drug and any benefit it has on heart failure is due to weight loss
Drugs in this class may have other effects that improve symptoms of heart failure
This study was too small and too short to draw big conclusions about a drug like this in heart failure patients.
I’m probably mostly in bucket 1, but I think that it’s reasonable to think that there may be more going on here.
On one hand, it’s really tempting to look at the results and say that it’s just all about the weight loss.
But on the other hand, when you dig into the data more, especially if you look at STEP-HFpEF DM as being related to STEP-HFpEF, some other ideas take hold.
Look at some of the letters to the editor after the STEP-HFpEF trial was published.
One of the most interesting comments has to do with how this class of drugs helps our bodies handle salt - there’s at least some evidence that drugs like Ozempic may have an effect that makes us urinate out sodium, similar to the impact a diuretic would have.
And ultimately, you shouldn’t make global changes in your practice pattern based on any one clinical trial, especially when it’s a small study that doesn’t follow patients for years and isn’t big enough to give you a sense of the impact on things like major adverse cardiovascular events or death from any cause.
One other big point that I’ve made before that this study reinforces: energy toxicity is a big deal, and this class of drugs is changing the world
Drugs in the GLP-1 agonist class5 help us navigate the modern world by impacting the way that our brains sense hunger.
The impact that we’ve seen on cardiovascular disease, diabetes, weight loss, and likelihood of dying from these drugs is almost unbelievable, but it’s consistent and cause for a significant amount of optimism.6
There is some speculation that the benefit we see here is because heart failure with a preserved ejection fraction is actually a metabolic disease, which makes sense to me.
We all have internal frameworks for how we think about the diseases that we treat.
One of my working internal thoughts about HFpEF is that it’s the equivalent of metabolic syndrome of the left ventricle and so it makes sense internally to me that treating metabolic syndrome will make this problem better.
But it’s vital to remember that just because we have an internal framework about a problem doesn’t mean that it’s accurate.
As of now, the data that we have suggests there’s some plausibility to this argument, but that’s all it is - biologic plausibility.
The modern environment is toxic on our bodies - too many calories, too little movement, too much stress, and so many other things - and drugs like Ozempic seem to make it a little bit easier for us to navigate.
The evidence keeps mounting here, and I continue to be bullish on the use of these medications.
Technically they used Wegovy and not Ozempic, but these drugs are the same thing despite having different names. Same active ingredient and same dosing. One is just marketed for obesity and one for diabetes. American health care is often stupid, this is just another example of how.
It’s also often challenging to diagnose because there’s no single blood test or imaging test that can make a diagnosis of heart failure. Heart failure is a clinical syndrome, which means that you make the diagnosis based on an assessment of symptoms, exam findings, and laboratory/imaging data.
The difference between STEP-HFpEF DM and STEP-HFpEF is that one looked a patients with diabetes and HFpEF while the other didn’t.
A lot of studies that look at so-called “hard endpoints” also measure quality of life, so it’s not like this is a foreign concept in a heart failure study
The more accurate term here is “incretin mimetic,” because some of these drugs impact more than just GLP-1
It’s worth noting that the evidence really suggests that tirzepatide (Mounjaro, Zepbound) is likely a better drug than semaglutide (Ozempic, Wegovy), which I wrote about here with some ideas why that might be the case.