



Some of the most important drugs that we use in medicine are blood thinners.
These drugs treat life threatening medical issues like heart attacks, strokes, deep vein thrombosis, and pulmonary embolism.1
I frequently tell my residents that I don’t buy the free lunch argument when it comes to blood thinners - there’s no drug ever developed that decreases the risk of blood clotting without necessarily increasing the risk of a bleeding complication.
And so when it comes to blood thinners, the question of “does the benefit outweigh the risk?” can be a pretty challenging clinical problem to decide about.
These drugs are life saving when used correctly, but can also be life threatening if their use leads to serious GI bleeding or intracranial bleeding.
The process of risk triangulation in blood thinners is a vital question to answer, and it’s also one that has big money on the line.
That’s why the recent news that Novartis just purchased Anthos pharmaceuticals caught my eye.
Anthon is a company that developed a drug called abelacimab, which blocks the function of a protein involved in blood clotting called factor XI.
Some people think Factor XI inhibition is the holy grail of blood thinners: a drug that reduces the risk of abnormal blood clots and doesn’t cause any increased risk of serious bleeding complications.
Inhibiting Factor XI with drugs mimics a natural outlier that has a low risk of blood clots
People born with Factor XI deficiency have a lower risk of blood clots, strokes,2 and probably heart attacks than the general population.
They also don’t seem to have an increased risk of serious bleeding complications or be abnormal in other ways.3
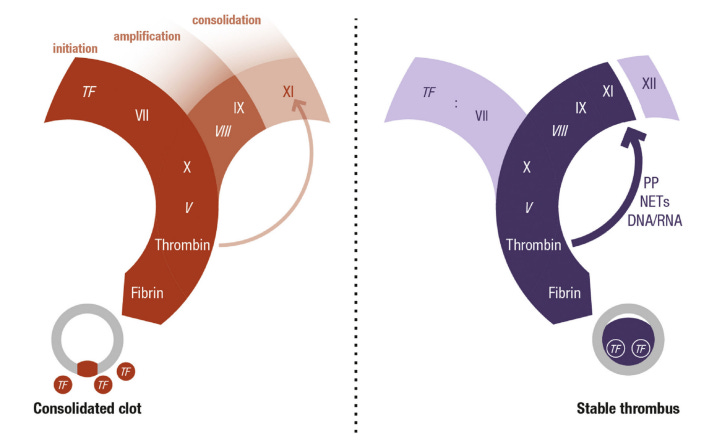
This may be because Factor XI is important for propagating a blood clot but not forming one.
Factor XI has a major role in pathologic blood clotting but only a minor role in allowing a blood clot to form in response to injury:
And so the basic science and observations of natural outliers raises the possibility that a drug that inhibits Factor XI could actually be the first class of blood thinners to successfully reduce the risk of strokes and pulmonary emboli without increasing bleeding risk like other blood thinners.
But it’s important to remember that a theoretical biological mechanism doesn’t actually prove a drug will be successful when it’s tested, so we need to look at the clinical trials before we really know anything.
Until recently, I thought that inhibiting Factor XI was a failed therapeutic strategy
The drug Asundexian, a factor XI inhibitor, was tested in the OCEANIC-AF trial, where it was found to be inferior to Xarelto in reducing stroke in patients with atrial fibrillation:

The data from this trial was so bad, that they stopped the trial early for lack of efficacy, and Bayer stopped their development of this drug that was supposed to be a blockbuster.
After OCEANIC-AF, I was ready to throw out the concept of Factor XI inhibition, but then I learned a bit more.4
It turns out that there is a real question of whether the problem with OCEANIC-AF was that inhibiting factor XI doesn’t work, or simply whether asundexian wasn’t effective it.
It turns out that asundexian didn’t inhibit factor XI all that well, at least at the doses tested in this study.5
Which brings us to why Novartis was interested in Anthos therapeutics.
A new drug that blocks Factor XI shows promise in a phase 2 trial
The drug abelacimab seems like it inhibits Factor XI much better than asundexian and also very clearly reduces bleeding risk compared to Xarelto:

Abelacimab is the reason why Novartis wanted to buy Anthos - there is real promise here that Factor XI inhibitors will supplant drugs like Eliquis and Xarelto as a superior class of blood thinner.
This has the potential to be huge news for patients and a gigantic windfall for the companies that develop these drugs.
But it’s worth being careful - until we have data that these drugs actually prevent strokes or treat DVTs, Factor XI inhibition is going to remain a theoretical solution rather than a practical one.
I’m very excited about the possibilities here, but the history of drug develop suggests that we should be tempered until we have data on the important outcomes that we care about.
There are a few lessons here that I think are applicable across domains of medication
The story of Factor XI inhibition highlights a few different concepts that I want to reinforce.
First, it’s time consuming and difficult to study something when you don’t have a perfect surrogate outcome and you need to power a trial for rare but scary events.
It would be so nice if we could infer safety and efficacy of a drug from measuring a few different biomarkers - levels of Factor XI, LDL-cholesterol, hemoglobin A1c - and just following patients for a short time.
But we can’t, certainly not with regards to a blood thinner.6
Antithrombotic therapy (the medical term for blood thinner) is one of the few things that we do medically that we don’t measure the effect.7
Can you imagine using a blood pressure medication but then not being able to check what someone’s blood pressure was?
That’s kind of how we approach most blood thinning medications in the real world, which is why an outcomes trial is vital before we start using these medications.
Second, natural outliers are one of the most important inspirations for drug discovery that we have.
Hopefully we will soon be able to add Factor XI deficiency to PCSK9 loss of function as a natural outlier that provided the outline for an important drug that saves lives.
And lastly, if you don’t understand the nitty gritty details, you’re going to get a lot of things wrong in medicine.
I was totally ready to just throw out the Factor XI inhibitors as a failed drug class after OCEANIC-AF, but that’s only because I didn’t have a clue what I was talking about.
Be careful about your voice of wisdom on any topic, because if they don’t truly understand what’s going on, then even when they’re right it’s by accident.
And so as I’ve dug into the details here, I am really excited about the promise that the Factor XI inhibitors may finally be the holy grail of blood thinners.
These are some of the most commonly prescribed drugs in the world. Things like Eliquis, Xarlto, Plavix, Brilinta, Coumadin are on this list. Even little old aspirin is a blood thinner. The nature of which blood thinner you use depends on which blood clotting problem you’re interested in treating - you use different drugs with different mechanisms depending on the medical issue.
Lower risk of stroke is seen even when they have atrial fibrillation.
Some of these patients do seem to have increased risk of bleeding after surgery or trauma.
The concept of “the further out you go, the deeper the water gets” is a profound point of learning that continues to be reinforced the longer I practice medicine.
There’s a comparison to be made with Factor XI inhibition to CETP inhibition for heart disease. The first drugs that blocked CETP were total duds, but the problem was that we didn’t understand the biology well enough. It’s why obicetrapib is the most exciting heart disease drug on the horizon.
The biomarker concept is part of why most of the “longevity” field is full of scam artists and bullshit. When you don’t have a good biomarker to evaluate something, it’s very hard or impossible to assess whether an intervention is working. You can’t manage what you can’t measure. And so when someone promises you a solution without a way of figuring out if it’s working, caveat emptor.
The exception here would be INR levels for patients on warfarin. But for patients who take Eliquis, or Brilinta, or aspirin, we just assume that these drugs work like magic. We don’t actually measure anything.