
Statins and the Misinformation Question: A Response to Sensible Medicine

There was a minor controversy on Med Twitter this week about a clip from Dr. Aseem Malhotra being interviewed by Joe Rogan after his confident statement that statins after a heart attack add “just over 4 days” to your life expectancy over five years.
It’s easy to watch that clip and become convinced that your cardiologist has been lying to you.
But interestingly the content in the clip is not the controversy that stirred up Med Twitter. The controversy is about whether that statement is “misinformation” or not:


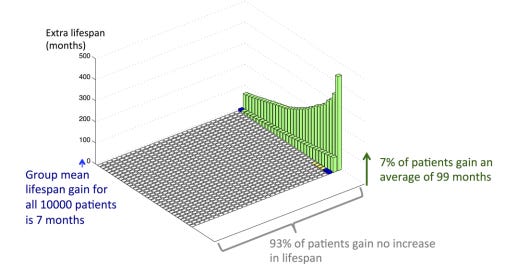
John Mandrola, whose work I has been very influential to me and read consistently, wrote a thoughtful response at Sensible Medicine. His argument: the “4 days” claim isn’t really misinformation. The Danish meta-analysis Malhotra cites is real and his math checks out. The benefit of statins for prevention isn’t evenly distributed - some people will get a huge benefit (i.e. if a statin prevents a heart attack, it can add decades to your life) and many won’t see much benefit at all (i.e. if you weren’t going to have a heart attack, the statin isn’t doing much:

Calling it misinformation, Mandrola warns, is how medicine loses trust.
It’s a really interesting statement, and I think he’s right about the fact that the way that doctors communicate about complicated health questions matters a lot.
It’s not just about the data. It’s also about the level of confidence, the room for disagreement, and other aspects of these challenging, nuanced decisions, which the medical profession hasn’t always been great at discussing in a public forum.
And since this discussion was so prominent among doctors I respect (and even made its way to in person in-hospital conversations this week), I wanted to add my two cents to the conversation about statins, misinformation, and the challenges of communicating about cardiovascular disease prevention.
The most important question for me that remains unanswered - Why do statins get treated as categorically different from antihypertensives?
This is one of the fundamental questions related to every single statin controversy that I think is fascinating.
After all, hyperlipidemia is a cardiovascular risk factor just like hypertension is a cardiovascular risk factor.
Nobody argues that you shouldn’t treat a primary prevention patient’s blood pressure because it’s asymptomatic, or because the absolute risk reduction in any given year is modest, or because some patients will be treated without individual benefit.
We accept that blood pressure is a risk factor worth paying attention to. And when someone has elevated blood pressure, we have a conversation about whether the risks of treatment outweigh the benefits.
The Francis et al. modeling paper that Mandrola cites, which shows that 93% of men on a preventive therapy gain no extra lifespan, applies equally to antihypertensives.
Should we stop treating hypertension in primary prevention? Of course not.
The asymmetry that Mandrola correctly identifies works the same way in both cases: miss a heart attack at 51 and you lose three decades; have a medication side effect and you stop the pill and move on with your life.
And yet nobody goes on Joe Rogan to say that lisinopril is a pharmaceutical industry scam. Nobody has built a career convincing patients to stop their blood pressure medications. The controversy is specific to statins, and that specificity is really interesting.
Why Statins Are Specifically Controversial
The statin controversy exists because of a deeper disagreement about whether cholesterol causes heart disease at all. I’ve written about this before - what the cholesterol skeptics get right, and what they get wrong - so I’ll keep this brief and link to those pieces.
The people who do not believe (or who cynically pretend not to believe) the lipid hypothesis of heart disease ignore a lot of important data to make their arguments. The most clever folks in this group will dress up their arguments with a ton of scientific detail, but they are fundamentally cherry picking the evidence.
The lipid hypothesis - that cholesterol containing particles get into the walls of blood vessels and cause inflammation and heart disease - is one of the aspects of modern medicine that we have the strongest level of confidence in.
It remains a hypothesis, but the evidence is pretty compelling:
Genetic variants that raise LDL increase heart disease risk tremendously
Genetic variants that lower LDL lower heart disease risk tremendously
Multiple different medications that lower LDL also lower cardiovascular risk and the degree of risk reduction is proportionate to the degree of lipid lowering
To reject the lipid hypothesis, you have to explain away way more than just the statin trials.
And the most sophisticated critiques - that LDL is necessary but not sufficient, that inflammation and insulin resistance and cumulative exposure all modify risk - are compatible with the lipid hypothesis, not contradictory to it.
So why does the controversy persist?
Largely because of the low-carb diet community, with whom there’s substantial overlap among lipid hypothesis skeptics. Low-carb diets frequently raise LDL. In fact, I’ve written about that impact in detail before.
If you feel dramatically better (or lose weight, or put your diabetes into remission) on a low-carb diet and then learn your LDL went up, you face an uncomfortable conclusion: either the diet that’s clearly helping you may also be hurting you, or the whole premise is wrong.
One of the most interesting disagreements about the lipid hypothesis comes from the perspective of the Paleo diet community. Their argument is that a low carb diet like the one we evolved to eat can’t possibly be bad for us.
This is wrong for a couple of reasons:
A modern Paleo diet doesn’t really resemble a true hunter-gatherer way of life. It’s higher in saturated fat, the modern Paleo diet gets way less fiber and indigestible plant matter, and hunter-gatherer populations move around way more than modern humans.
Cardiovascular disease won’t be impacted by natural selection, so even a diet we evolved to eat is compatible with a diet that increases cardiovascular risk. We develop heart disease long after reproductive years, so genes that very clearly increase heart attack risk - like Lp(a), for example - never get outcompeted and filtered from the gene pool.
A lot of people simply believe the lipid hypothesis can’t be true because it conflicts with other beliefs and work backward from there. That’s understandable.
Statins Are Just Drugs
The most impressive sociologic success of the anti-statin crowd is to elevate these medications to a level of menace they shouldn’t occupy.
Statins are pretty boring drugs. If you take one and develop muscle symptoms, you stop it and the symptoms resolve.
Thiazide diuretics (a common treatment for hypertension) can worsen insulin sensitivity - just like statins do - but nobody is building a movement around the dangers of hydrochlorothiazide.
The asymmetric scrutiny is a product of motivated reasoning, not pharmacology.
It’s also worth knowing that prescribing statins is a financial loser for doctors.
Generic statins cost pennies. I make nothing from the prescription.
It would be so much more lucrative for most doctors to skip the conversation about lipid lowering and just see another patient. It takes a lot of time and focus to explain the data, navigating the social media discourse, and have a nuanced conversations about personalized risk.
But I have these conversations because I find the evidence that statins lower risk of heart disease to be persuasive.
On Malhotra Specifically
Most of Med Twitter was focused on the discussion about whether Malhotra’s points on Joe Rogan were “misinformation,” but to understand this discussion, you need context about Aseem Malhotra.
The “4 days” figure that he cites comes from real data. But technically correct statements can still be deliberately misleading.
When we think about Dr. Malhotra, we have to remember the historical context - this is someone who has built an entire career and substantial income telling people statins are poison.
I’m not going to spend too much time talking about the methodological reasons why Malhotra’s specific argument is so cynical and misleading - read the Twitter feeds of Dr. Ethan Weiss or Dr. Darrel Francis for the details.
But it’s notable that in 2026, when the lipid hypothesis is much stronger than when Malhotra originally became prominent, that this Rogan clip actually represents a kind of evolution: he’s no longer claiming statins don’t work or kill you. He’s now conceding they’re lifesaving but arguing they’re not as lifesaving as sometimes described.
Presenting a five-year trial’s average survival gain without context to an audience of millions with no framework for interpreting it is a conscious choice.
It is not the choice that someone genuinely trying to help people understand their cardiovascular risk would make.
To borrow from Upton Sinclair: it is difficult to get a man to understand something when his salary depends on his not understanding it.
Mandrola worries that calling things misinformation when they’re technically true erodes trust in medicine. He’s right. But I’m not sure it’s right to be extending professional courtesy to this type of deliberate obscuration and calling it nuance is the right counterbalance.
In medicine, we use Bayesian reasoning to try to make sense of new information. We use our prior assessment of a situation to interpret the likelihood that new data has validity. With Malhotra, we have a long history of someone deliberately obfuscating the lipid hypothesis and the benefit of statins. So my pre-statement probability that he is honestly assessing the data and not cynically manipulating the numbers to make a predetermined point is quite low.
And as a consequence of this context - Malhotra spending years basically accusing doctors of trying to harm our patients by giving them statins - is that a lot of physicians took issue with Mandrola’s decision about what battle to fight.
What the Conversation Should Actually Look Like
None of this means every primary prevention patient should be on a statin.
It certainly doesn’t mean that anyone “needs” a statin.
The lottery framing that Mandrola uses is honest and worth considering. But the asymmetry and unpredictability is worth explaining in detail: if you’re the one who avoids a massive MI at 55, you might gain thirty years. If you develop side effects, you stop the medication.
We don’t know if you’ll be in the group that benefit or the group that doesn’t. But we do have a sense that risk has randomness to it. But if you have a heart attack prevented, you may gain decades (and if you have a side effect, we can just stop the drug).
But that conversation - quantitative, contextual, individualized - is the same one we have about blood pressure.
We don’t reserve it only for lipids, and we don’t let technically-true-but-misleading statistics convince us that treating hypertension is a scam.
I believe we should treat elevated LDL the way we treat elevated blood pressure: as a modifiable cardiovascular risk factor, with cheap and generally well-tolerated medications, in the context of an honest conversation about who benefits and how much.
Do that, and most of this controversy dissolves. What remains is a man who figured out that criticizing the motives of doctors is more profitable than practicing good medicine.
Previously on this topic: Everyone Has an Opinion on Statins | What the Cholesterol Skeptics Get Right | What They Get Wrong | Preventive Medicine = Overtreatment?
Patient's perspective here:
I've never had a nuanced discussed with my PCP about medications (or pretty much anything else). The same is true of pretty much everyone I've discussed this big-picture issue with. So while I appreciate the care that it appears that you and some of the commenters here show with patients, that might be the exception.
As for statins in particular, my experience reinforces the general point I made above: I'm a 61-year-old male, a daily runner for 47 of them, weigh what I did in college, no symptoms of chronic disease. My LDL is high enough that it ranks as "elevated." My PCP has twice (via his employer's message portal, not in person) said this means I should be on statins. No discussion of options, no discussion of how the LDL relates to my HDL and triglyceride numbers (which are in the "excellent" range). He knows I run a lot, so he's not going to recommend being more active. But we've not once discussed diet or any other factors. (I weigh 130, so between that and the running he probably thinks I live on oak bark.)
So I just wanted to provide a little insight why some (who have nothing to do with Paleo, etc.) are skeptical. This guy looks at one number and immediately starts talking about medication. Ideally, I would ask, "Can you show me data on people in my demographic with my numbers and activity level and symptoms, and show that statins made a significant difference in MI risk compared to those who didn't take them?" But come on, I get 15 minutes with him once a year. There's no point in even asking the question.
I think a contributing factor might be that the average layman is not educated in either research design or in statistics, and I wish these topics (at a basic level) were mandatory in high school. Patients only care about what will happen to THEM, while doctors base intervention decisions on population level data because currently, they don't have a sufficiently accurate prediction model as to who will benefit and who will not. For those with high LDL but hesitant to take a statin, getting a CAC score could help. (Seeing the atherosclerosis in my heart was very motivating!).
As for individualizing treatment decisions, there is one thing that CAN be done (but usually isn't). When I first went on a statin, even a high dose was not enough to sufficiently lower my LDL, and my liver enzymes were elevated. Luckily I listened to a podcast with lipidologist Dr. Thomas Dayspring and learned about the Cholesterol Balance Test from Boston Heart, which can be ordered online from Empower Dx and taken at home. The test indicated that I was a cholesterol hyperabsorber, and thus Ezetimibe would work better for me than a statin (and it has, although I still take a low dose statin, since absorption and production can adapt somewhat in a homeostatic manner). Ezetimibe is as cheap as a statin and without the same side effects, and works better than a statin for the roughly 20% of us who are cholesterol hyperabsorbers. Why don't more doctors seem to know this?
https://www.ahajournals.org/doi/10.1161/JAHA.123.031865
https://bostonheartdiagnostics.com/wp-content/uploads/2023/06/02031115-CBT-Treatment-Algorithm_160108.pdf