
The New Cholesterol Guidelines Are Here. Take a Deep Breath

I got more questions about the new cholesterol guidelines in the past few days than I get about most things in medicine.
Friends, patients, colleagues, family members, all curious about what this means.
My favorite was: “Omg new lipid guidelines. Is this like your Christmas?”
I understand the interest.
When a major guideline document gets released, it feels like something brand new and super important just happened. The news cycle certainly treats it that way. The headlines scream about new targets, new tests, new recommendations.
But before we get into the details, it’s important to remember: nothing new was discovered this week.
The 2026 ACC/AHA Dyslipidemia Guideline is not a study or a trial result. No experiment was run. No patients were randomized.
The guidelines are the product of a group of experts diving deep into the research on cholesterol treatment, much of which has been published for years, and negotiating1 about what it means for clinical practice.
That’s an important and valuable exercise with significant impact. I’m not dismissing it.
But the doctors who live in this space - preventive cardiologists, lipidologists, and internists who are reading every trial as it comes out - have been constantly integrating this information into how we think about patients and how we practice.
We have been doing this in real time and the guidelines are catching up to where many of us already are.
And so there’s something artificial about the news cycle this week.
Remember, guidelines aren’t commandments from above written on stone tablets. They’re the product of a group of smart people, with their own perspectives, biases and conflicts of interest, who hashed out a negotiated interpretation of the evidence.
Reasonable people can (and do) look at the same information and come to different conclusions. There’s a reason that a “second opinion” has such medical longevity.
With that framing, let me walk through what I think the guidelines get right, where they fall short, and why I have real concerns about how they’ll be implemented.
What I Like
Emphasis on lifetime risk and area under the curve.
The most important takeaway from the guideline writers is that we should think about treating high cholesterol earlier to reduce lifelong risk.
This tracks with the direction that most people in the field approach understanding risk - cholesterol related cardiovascular risk is cumulative, it’s about exposure and time.
It also tracks strongly with how I take care of patients.
In general, I am a believer in the ALARA principle for LDL levels. ALARA stands for “as low as reasonably achievable,” a term stolen from the radiation safety literature.
The definition of what constitutes “reasonable” will depend on someone’s overall risk, their medical and family history, their personal preferences, and their willingness to consider prescription medications and to implement dietary changes.
Reasonable for one person does not necessarily mean reasonable for another. But the guidelines clearly get it correct that lower for longer is likely better2 and we should be integrating time exposure into our counseling and treatment approach.
Lp(a) measurement is formally recommended
I am of the belief that checking Lp(a) is helpful for many patients, only because it serves as a tiebreaker for a lot of other clinical decisions that we make - when Lp(a) is high, I am more likely to recommend treating LDL, or hypertension, or starting a GLP-1 medication, particularly when someone has a family history of cardiovascular disease.
Now, some people will disagree about the value of this test since we don’t have targeted treatments for it, but I think the guidelines got this one right.3
Non-statin therapies get formal recognition
The era of statins-only is over. Ezetimibe, bempedoic acid, and PCSK9 inhibitors are codified as next steps when statins alone don’t get the job done. This connects to what I wrote about the VESALIUS trial - for high-risk patients, we have compelling evidence that more aggressive lipid lowering works, and we shouldn’t be waiting for a heart attack to use the tools we have.
ApoB gets a seat at the table
The guidelines acknowledge that apolipoprotein B can be useful for assessing personal risk, particularly in patients with metabolic syndrome, diabetes, or high triglycerides. But I think it somewhat underplays the best biomarker for lipid related cardiovascular risk.
In my clinical work, I prefer to check apoB for almost all patients to understand whether their apoB is concordant with their LDL-C, because when they don’t match up, apoB is a better biomarker.
The guidelines here are pretty good, and I agree with a 2a recommendation based on the level of evidence that we have. I might go a bit farther to emphasize the concept of LDL-apoB concordance and discordance more than they do, but that’s a minor quibble.4
Where I Have Problems
The evidence quality gap
Jim Stein - a preventive cardiologist whose Substack I’d encourage everyone to subscribe to - wrote an important critique of the guidelines the day they were published.
His hottest take (which I cosign) is that there’s a hubris problem with the guidelines.
Roughly 70 recommendations carry the strongest possible designation (Class 1, meaning “is recommended” for virtually all appropriate patients), but only about 20% of those are backed by the highest quality evidence from multiple randomized controlled trials.
Nearly half of the strongest recommendations are based on pretty low quality data.5
That’s a problem. When a guideline says “is recommended” with Class 1 confidence, it becomes the standard of care.
I can’t tell you how many conversations I’ve had with other doctors where “what the guidelines say” is thrown about as a justification for decision making without digging into any of the underlying data that informs those guidelines.
Too many doctors treat a Class I guideline recommendation as settled science, and so guideline recommendations filter down to the medical care that most people are receiving.
And it’s not just doctors. Payers listen to those recommendations. Health systems build protocols around it. The media reports it as what we should do.
When the underlying evidence is observational - data that can’t establish causation - the gap between the confidence of the recommendation and the quality of the evidence is misleading.
This is something I care deeply about: the calibration between how certain we are and how certain we should be.
The risk calculator problem
The guidelines recommend replacing the old Pooled Cohort Equations with the newer PREVENT-ASCVD calculator for 10- and 30-year risk estimation.
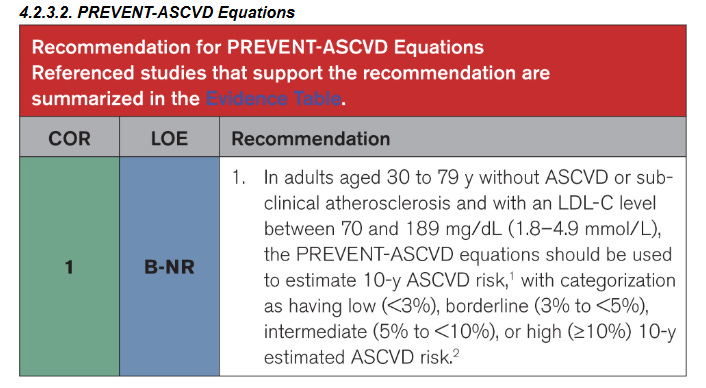
PREVENT is certainly a better risk calculator. It adds kidney function, hemoglobin A1c, and BMI. That’s an improvement.
But overall, risk calculators kind of stink and I have a fundamental problem with any guideline that emphasizes risk calculators for individual decision making in day-to-day clinical practice.
For one thing, they all use age as a dominant input variable, which means that they systematically miss young people who are at genuinely elevated risk - the 38-year-old with a strong family history and an Lp(a) of 250 nmol/L - and systematically flag older people for treatment who are going to be fine no matter what we do.
Risk calculators work well across populations, but too often they’re presented as though they work well for individual patients.
They don’t. They create an illusion of precision that doesn’t exist.
The fundamental limitation of any guideline that leans heavily on risk calculators is that it encourages doctors to outsource clinical judgment to a number with wide confidence intervals, derived from populations that may not resemble the person sitting in front of them.6
In practice, these guidelines lead to too much medicine-by-algorithm and over-medicalizing people
These are my biggest critiques of the guidelines, and they manifest in three specific ways.
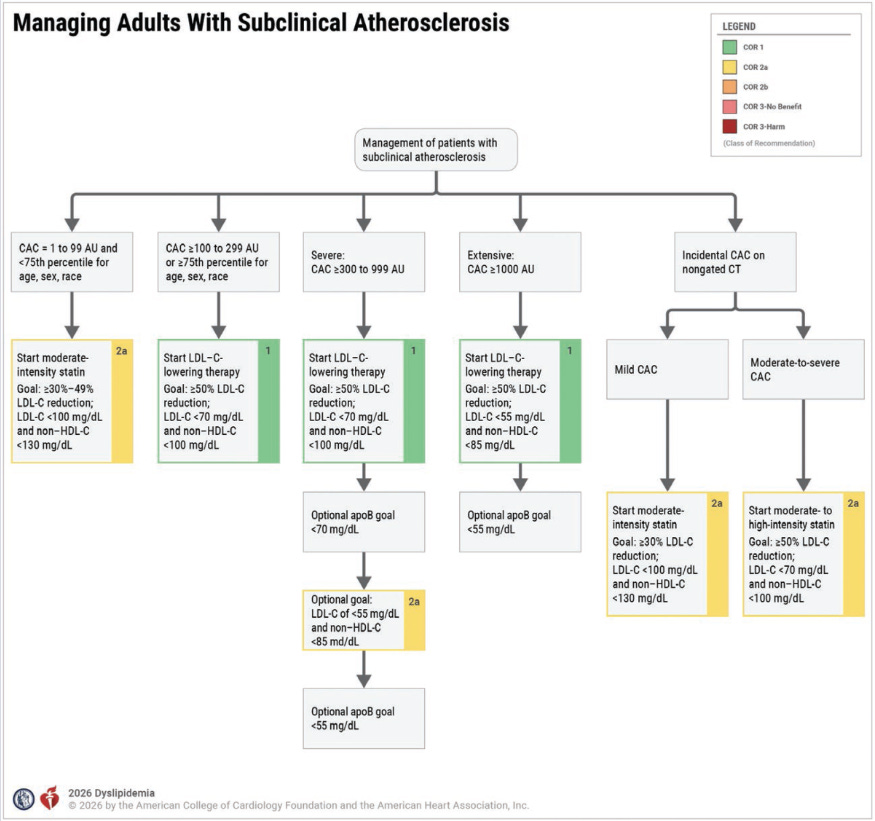
The use of calcium scores and the arbitrary cutoffs on their interpretation
The guidelines assign different treatment recommendations based on coronary artery calcium (CAC) score thresholds and say that any CAC above zero supports treatment, with progressively lower LDL targets as the score rises.
One problem is that this creates arbitrary cutoffs that aren’t truly meaningful - a calcium score of 99 is not fundamentally different from a calcium score of 101 just like a score of 280 is not meaningfully different from 320 or the 70th percentile is not meaningfully different than the 82nd.7
But the algorithmic nature of these recommendations is going to lead to a lot of mediocre medicine with doctors looking at a number, plugging it into a flowchart, and following the recipe instead of thinking about the whole patient:
And I have a bigger problem with the CAC emphasis than just the cutoffs.
The guidelines give CAC a Class 1 recommendation even though no randomized controlled trial has proven that a CAC-driven strategy reduces cardiovascular events compared to not testing.
The recommendation converts a prognostic association (people with more calcium tend to have more events) into a treatment algorithm (people with coronary calcium should be treated in this specific way).
Those are not the same thing.
Moreover, a calcium story fundamentally misses the mark in young people. A calcium score of zero in a 35-year-old is not the reassurance that it’s sometimes made out to be.
I’ve seen dozens of young patients with calcium scores of zero who have clear coronary disease on CT angiography or who have had hart attacks.
“The power of zero” is a myth, and recommending CAC as a primary screening tool has the potential to cause harm with false reassurance and, on the other end, a lot of unnecessary downstream testing, including stress tests and catheterizations that don’t help patients.8
CAC is one piece of the puzzle. It is not the puzzle.
Statin intensity labels kind of miss the point
The guidelines categorize lipid-lowering therapy by intensity (high, moderate, low) based on the specific drug and dose.
This introduces unnecessary complexity into clinical decision making. Take a look at this table from the guidelines:
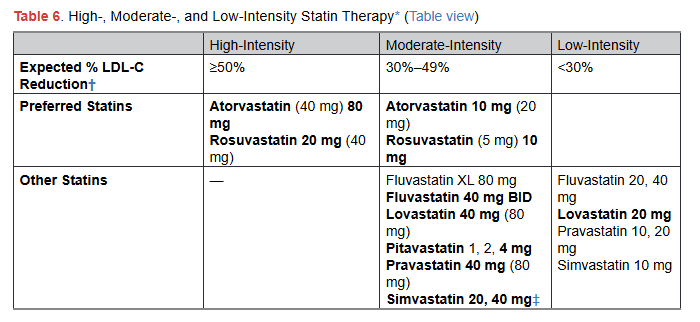
It’s really confusing!
One problem is that there’s massive heterogeneity in how people respond to statins. I have patients who get a 50% LDL reduction on 5 mg of rosuvastatin, and patients who barely budge on 40 mg.
And so if the guidelines recommend a high intensity statin as a Class 1 recommendation, but I start 5mg of rosuvastatin with a plan to monitor and increase if necessary, does that mean I’m practicing bad medicine?
The intensity of the prescription is a proxy for the response. And when you start treating the proxy as the thing itself, you might lose sight of what matters: did the patient’s numbers actually improve? I don’t think a focus on whether the prescription matches an arbitrary intensity cutoff more makes any clinical sense.9
Outstanding preventive care doesn’t work well with algorithms
The guidelines are overly prescriptive, too complicated, and too confident about what we should do for patients.
Consider a patient with an LDL of 65 whose guideline-recommended goal is 55. According to the algorithm, we should intensify therapy.
But what if their blood pressure is running 150/95? What if they have diabetes with an A1c of 7.9?
Sure, it makes sense to treat the lipids, but is that really the best next step? Or do you really want to be adding 3 different medications for someone in a single clinic visit?
Not to mention the fact that people often feel like you are throwing pills at them rather than performing a holistic risk assessment.
In the case of that patient, you get far more cardiovascular risk reduction from focusing on the blood pressure and diabetes than from squeezing another 10 points out of the LDL.
When guidelines emphasize treat-to-target, there’s a real risk that the target becomes the entire conversation. That’s cookbook medicine.
And at the same time I have a critique of the overly simplified approach, I also think that the guidelines are simultaneously too complicated: calculate risk using the PREVENT calculator, get a CAC score, start a moderate-to-high potency statin, get the numbers down 30-50%, or to a target of 55mg/dL.
That dichotomy - too algorithmic but also too convoluted - is part of why I struggle with what to do with these guidelines.
The Bigger Picture
The 2026 lipid guidelines are a reasonable document produced by smart people doing hard work.
Much of what they recommend reflects where the evidence has been pointing for years - lower LDL for longer is better, we have more tools than just statins, and lifestyle intervention should be the foundation.
But the guidelines are also an imperfect document that reasonable people can read and disagree with.
The news cycle around these guidelines creates a false impression that something fundamentally changed even though nothing did.
The best thing you can take away from this week isn’t a specific number or a new test or a revised flowchart.
So my answer to all of the people who asked me about the new guidelines is that these guidelines don’t change anything about how I’m taking care of patients.
What matters is understanding your individual situation - your labs, your family history, your imaging if we have it, your risk tolerance, your preferences - and making a plan based on that, not based on a flowchart.
Previously on these topics: Everyone Has an Opinion on Statins | VESALIUS and the New Line for Aggressive Prevention | Most Doctors Don’t Interpret This Test Correctly | The Pitfalls with Heart Disease Screening | Is Your Doctor Misusing Cardiac Testing? | Preventive Medicine = Overtreatment?
Thank you for reading! Please share with friends and family and encourage them to subscribe!
Disclaimer: This is my opinion, not medical advice. Reading this newsletter does not constitute the formation of a doctor-patient relationship and is no substitute for the opinion of your doctor.
Negotiating is the correct word here. Guideline are the result of a debate and discussion about different interpretations of the research. Producing a consensus document like this requires negotiation.
Although the authors acknowledge that we have a true knowledge gap about whether very early treatment strategies reduce lifelong risk. We think that they do, but that’s very different from having data that tells us that they do.
And the medications to treat elevated Lp(a) are in late stage clinical trials, so I am optimistic that we’ll actually be able to do something about this soon.
Concordance and discordance matter because LDL cholesterol measures the cholesterol carried by LDL particles, not the number of particles themselves. When the number of particles (measured by apoB) is higher than you’d predict from the LDL cholesterol, risk is higher. When it’s lower, risk is lower. I think that the traffic metaphor is best here. LDL tells you about the number of commuters, but apoB tells you about the number of cars on the road.
Low quality data doesn’t mean no data. It doesn’t even mean wrong data. It just means that the evidence isn’t based on randomized trials and they are based on either observational evidence or expert opinion.
And this problem also applies to “cardiac age” calculators that have gotten press before.
This is true of virtually all biological cutoffs, of course. But it’s particularly problematic when the guideline assigns meaningfully different treatment recommendations on either side of an arbitrary line.
James H. Stein, MD wrote about this in detail in his pieces “The Power of Zero Is a Myth” and “Why CAC Risk Reclassification Fails Clinically.” I’d recommend reading both. My clinical experience matches his analysis. Calcium scores are a blunt instrument, and the absence of calcium does not mean the absence of disease.
Patients also ask all the time why they are on such a high dose of a medication and whether they can decrease the number of milligrams.
For me I was always taught “Guidelines provide the map—but you still have to drive the car”.
Great post, Greg! You made so many good, patient-oriented points. I appreciate the shout outs, too! Your point about them being simultaneously too complex and too simple is really compelling. I think that point underlies my take-home that the entire process is broken: it's too broad in scope, too complex, insufficiently focused on patient preferences, and compromised by intellectual bias and industry relationships. A better process would require a higher evidentiary threshold for Class I recommendations, fewer recommendations overall, less redundancy and wordsmithing, clearer and more useful figures, and fewer authors with strong intellectual or financial stakes in the outcome. But I loved your other point too - nothing really changed (though I worry payers and lawyers will use this as fodder).